

Examining trends in the survival benefit of re-kidney transplantation over the past three decades
Shaifali Sandal1, JiYoon B Ahn2, Yusi Chen2, Allan Massie3, Marcelo Cantarovich1, Dorry Segev3, Mara A McAdams-DeMarco3.
1Internal Medicine/Nephrology, McGill University Health Centre, Montreal, QC, Canada; 2Surgery/Transplant, Johns Hopkins University, Baltimore, MD, United States; 3Surgery/Transplant, NYU Grossman School of Medicine and NYU Langone Health, New York, NY, United States
Background and objectives: A survival benefit to re-kidney transplantation (KT) has been demonstrated and the risk profile of patients being considered for re-KT is widening. Furthermore, outcomes of patients on dialysis have improved over time for those with a history of graft failure. Thus, we tested whether the survival benefit of re-KT has diminished over time.
Methods: Using SRTR data, we identified patients 25,397 patients who underwent re-KT from 1990-2019 and 25,397 waitlisted counterfactuals from the same year with the same waitlisted time following graft failure. We assessed the survival benefit of re-KT using the sequential stratification method. We tested whether this association differed by age at listing (18-64 vs. ≥65 years), and by era of listing (1990-99, 2000-09, 2010-19; pre- vs. post-KAS era [2010-14 and 2015-19).
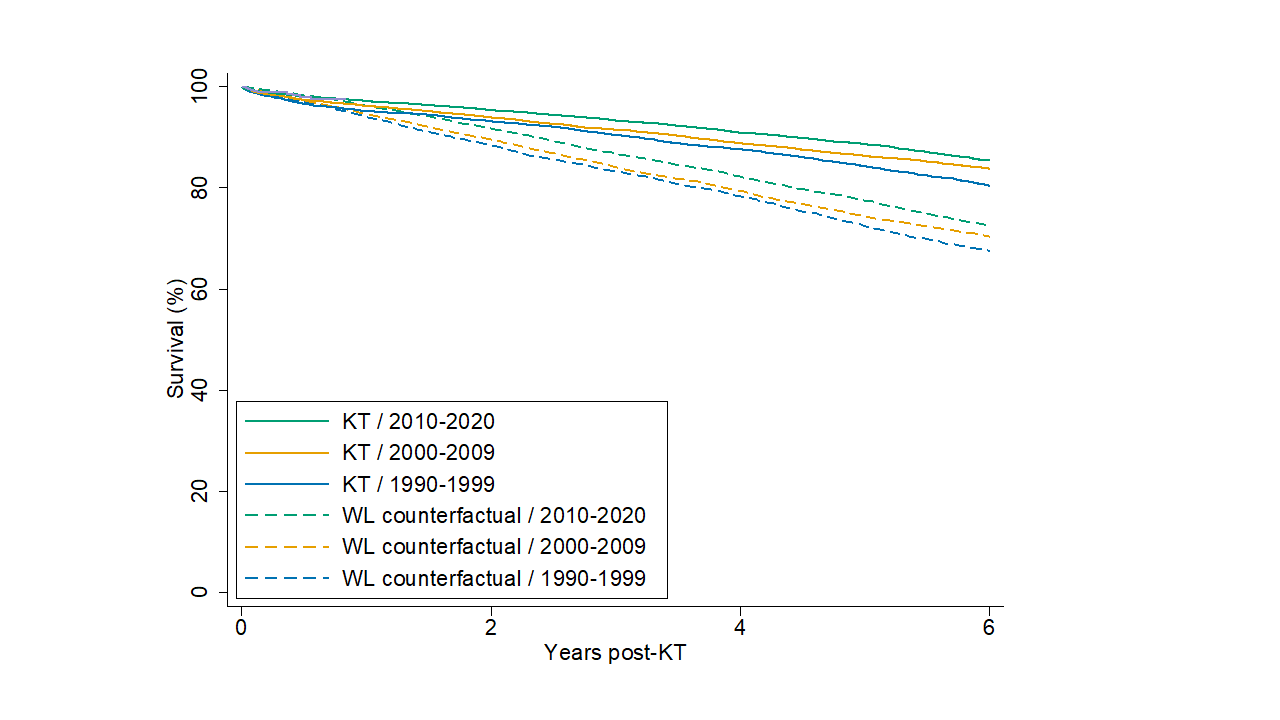
Results: Patients who received re-KT had a better survival than waitlisted counterfactuals (1-year:96.5% vs. 95.2%, 3-year:92.1% vs. 85.1%, 6-year:83.9% vs. 70.8%). In adjusted analyses, re-KT was associated lower hazard of mortality compared with waitlisted counterfactuals (aHR=0.62, 95%CI:0.60-0.64) and this association was not different by age at waitlisting (Pinteraction=0.30). When stratifying the analysis by era, the survival benefit of re-KT was noted in all three eras (1990-99:aHR=0.70, 95%CI:0.65-0.74; 2000-09:aHR=0.58, 95%CI:aHR=0.56-0.61; 2010-19:aHR=0.55, 95%CI:0.51-0.58) (Figure). Also, when compared with the 1990-99 era, the survival benefit of re-KT was higher in the 2000-09 and 2010-19 eras (Pinteraction<0.001 for both). Furthermore, during the KAS era, there was a survival benefit to re-KT (aHR=0.57, 95%CI:0.51-0.65) and which was higher than that observed in the pre-KAS era Pinteraction=0.004).
Conclusion: Re-KT is associated with a significant survival benefit when compared with waitlisted patients on dialysis and over time incremental increases in the survival benefit were observed. This benefit exists for older and younger adults. We recommend examination of current practices surrounding re-KT referral and candidacy and the development of guidelines and policies to increase re-KT among patients of all ages.
This study was supported by NIH R01DK120518 (McAdams-DeMarco) and K24AI144954 (Segev). Mara McAdams-DeMarco was also supported by R01AG055781 from the National Institute on Aging and R01DK114074 from NIDDK.

