
Outcomes of dialysis dependent second kidney transplant recipients by induction type in the United States
Kurtis J Swanson 1, Scott Jackson2, Raja Kandaswamy3, Samy Riad1.
1Nephrology , University of Minnesota, Minneapolis, MN, United States; 2Complex Care Analytics , MHealth Fairview , Minneapolis, MN, United States; 3Surgery , University of Minnesota, Minneapolis, MN, United States
Background: We examined the association between induction type for second kidney transplant in dialysis dependent recipients and the long-term outcomes.
Material and Methods: Using the Scientific Registry od transplant Recipients SRTR standard analysis file, we identified all second kidney transplant recipients who returned to dialysis prior to re-transplantation. Exclusion criteria included: missing, unusual, or no-induction regimens, maintenance regimens other than tacrolimus and mycophenolate, and positive crossmatch status. We grouped recipients by induction type into three groups: Anti-thymocyte group (n=9899), Alemtuzumab group (n=1982) and IL-2 Receptor Antagonist group (n=1904). We analyzed recipient and death-censored graft survival (DCGS) using the Kaplan-Meier survival function with follow up censored at ten-year post-transplant. We used Cox proportional hazard models to examine the association between induction and the outcomes of interest. To account for center specific effect, we included center as a random effect. We adjusted the models for pertinent recipient and organ variables.
Results: In the Kaplan-Meier analyses, induction type did not alter recipient survival (log-rank p=0.419) or DCGS (log-rank p=0.146). Similarly, in the fully adjusted models, induction type was not a predictor of recipient or graft survival. Live-donor kidney was a favorable predictor of recipient survival [HR 0.73, 95% C.I. (0.65, 0.83), p<0.001] and graft survival [HR 0.75, 95% C.I. (0.66, 0.85), p<0.001]. Publicly insured recipients had worse recipient and allograft survival outcomes.
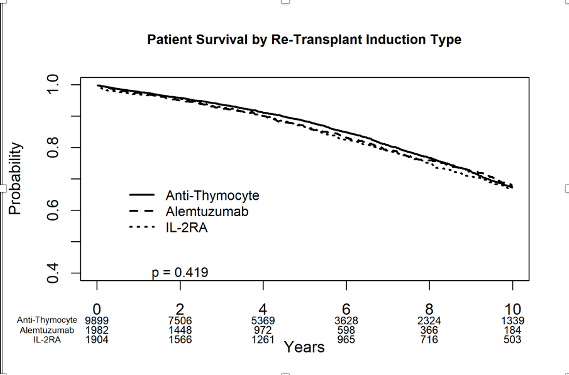
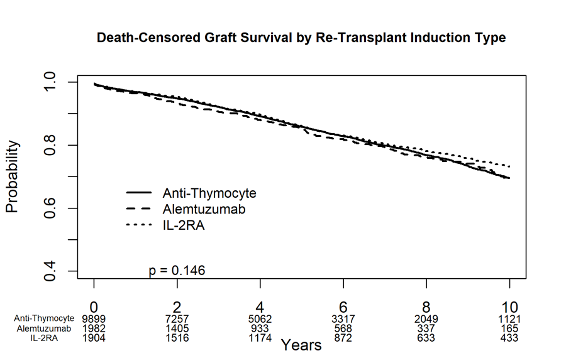
Conclusion: In this large cohort of second kidney transplant recipients, who were on dialysis prior to transplantation and discharged on tacrolimus and mycophenolate maintenance, induction type did not influence the outcomes of recipient or graft survival. Live-donor kidneys improved recipient and graft survival.

right-click to download