
Outcomes of preemptive second kidney transplant by induction type in the United States
Samy Riad1, Kurt Swanson 1, Scott Jackson2, Raja Kandaswamy3.
1Nephrology , University of Minnesota, Minneapolis, MN, United States; 2Complex Care Analytics , MHealth Fairview , Minneapolis, MN, United States; 3Surgery , University of Minnesota, Minneapolis, MN, United States
Background: The role of induction in preemptive second kidney recipients is unclear. We examined the association between induction therapy and the long-term graft and recipient survival in the settings of tacrolimus and mycophenolate maintenance.
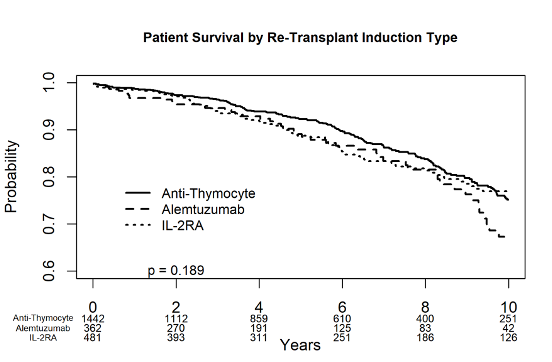
Methods: We identified all preemptive second kidney transplant recipients between 2000 and 2020 in the Scientific Registry of Transplant Recipients. We excluded those with missing or mixed induction regimens and positive crossmatch. We grouped recipients by induction type into three groups: Anti-thymocyte globulin (n=1442), Alemtuzumab (n=362), IL-2 Receptor Antagonist (n=481). We generated Kaplan-Meier curves of the recipient and death-censored graft survival (DCGS) with follow-up censored at ten years. We used multivariable Cox Proportional Hazards models to examine the association between induction and the above outcomes. We adjusted the models for recipient and donor variables.
Results: Rates of delayed graft function (DGF), rejection, hospitalization, and post-transplant lymphoproliferative disorder (PTLD) at one year were not statistically different. Recipient survival did not vary by induction type in the Kaplan-Meier analysis (log-rank P=0.189) or in the multivariable model.
However, DCGS was the lowest in the Alemtuzumab group (log-rank P=0.01).
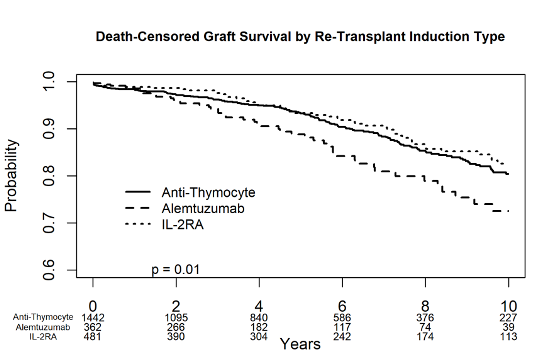
In the multivariable models, alemtuzumab was associated with a 57% increased risk of graft loss [1.57, 95% C.I. (1.08, 2.30), P=0.019] compared to anti-thymocyte. Live-donor kidneys were associated with significantly better recipient survival [aHR 0.67, 95% C.I. (0.51, 0.89), P = 0.005] and DCGS [aHR 0.55, 95% C.I. (0.40, 0.76), P < 0.001].
Conclusion: Compared to anti-thymocyte induction, alemtuzumab, but not IL-2RA, was associated with inferior graft survival in preemptive second transplant recipients discharged on tacrolimus and mycophenolate.

right-click to download