Sharing under KAS – what is the impact according to KDPI?
Molly Jacobs1, Robert Stratta1, Colleen Jay1.
1Surgery, Abdominal Organ Transplant, Atrium Health Wake Forest Baptist, Winston-Salem, NC, United States
Purpose: The Kidney Allocation System (KAS) implemented in 2014 changed prioritization of highly sensitized patients and other groups impacting sharing. We sought to determine effects on sharing according to Kidney Donor Profile Index (KDPI) across pre- and post-KAS eras.
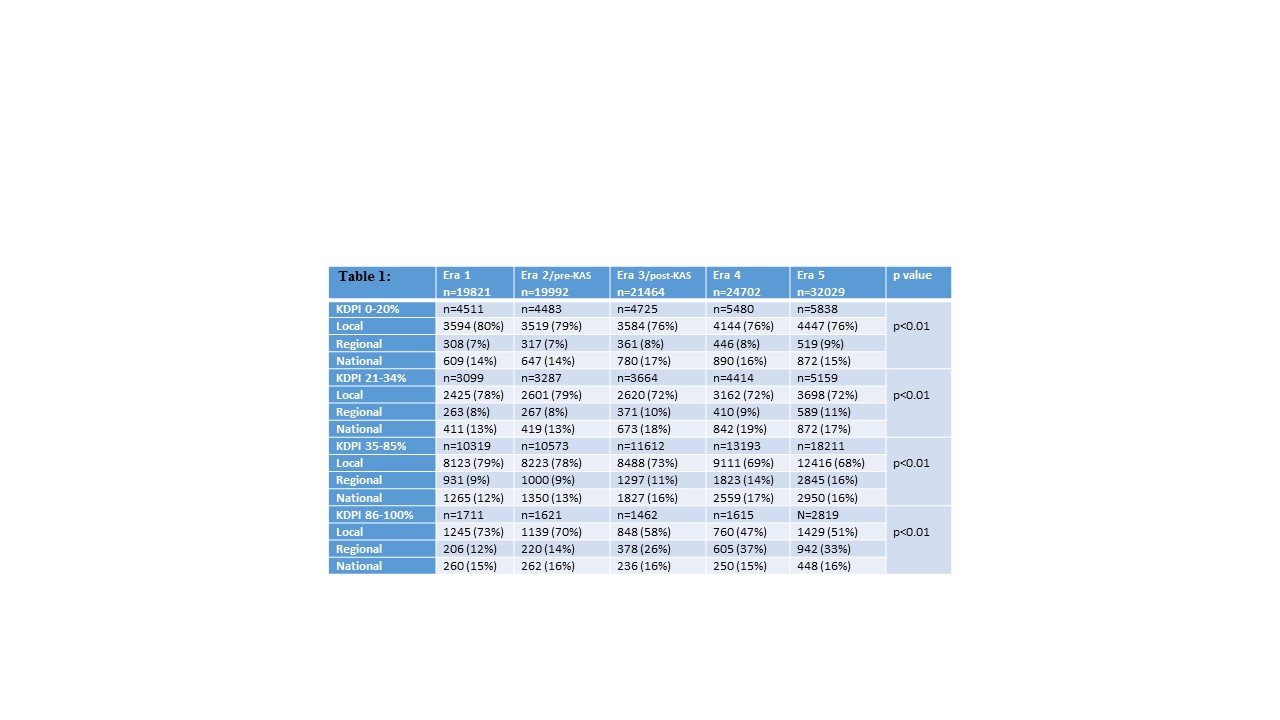
Methods: Using UNOS data, we compared local, regional, and national utilization for deceased donor kidney transplants (DDKT) alone according to KDPI group and KAS era: Era 1 (2010-2011, pre-KDPI), Era 2 (2012-2013, pre-KAS), Era 3 (2014-2015, early post-KAS), Era 4 (2016-2017), and Era 5 (2018-2020).
Results: Since KAS, sharing has increased across all KDPI groups, and is more pronounced with increasing KDPI. Regional utilization more than doubled for KDPI >85% kidneys while local use decreased 30% from Era 1 to 5 (Table 1). However, a 60% increase in absolute numbers of DDKT across eras resulted in higher local DDKT volume in Era 5 despite increased sharing. Sharing for calculated panel reactive antibody (cPRA) 99-100% patients increased post-KAS across all groups, but the effect was less pronounced for KDPI >85% (32% increase compared with 71-89% increase for the other 3 KDPI groups). Sharing for high cPRA patients accounted for only 23% of shared kidneys and 8% of DDKT in Era 5.
Conclusion: KAS increased sharing across all KDPI groups with the largest change occurring in regional use of KDPI >85% organs. Higher DDKT volumes over time offset any changes in sharing such that local volumes for all KDPI groups increased. Increased sharing for cPRA 99-100% occurred across all KDPI groups, but represents a minority of kidneys shared.