
Gram negative blood stream infection in renal transplant recipients: risk factors and outcome from a transplant center in Pakistan
Sunil Dodani1, Asma Nasim1, Tahir Aziz2.
1Infectious Diseases, Sindh Institute of Urology and Transplantation, Karachi, Pakistan; 2Transplant Nephrology, Sindh Institute of Urology and Transplantation, Karachi, Pakistan
Background: Gram-negative bacteremia (GNB) is a common cause of bloodstream infection in renal transplant recipients (RTR). The risk factors are cytomegalovirus infection (CMV), pre-transplant dialysis, acute rejection, urological abnormalities, and ureteral stent. The mortality rate is 2.5 to 11%. Considering the huge impact on morbidity and mortality, our aim is to analyze the characteristics and outcomes of GNB in RTRs.
Methods: A case-control study at Sindh Institute of Urology and Transplantation (SIUT), Karachi, Pakistan. The files of all renal transplant recipients who had documented GNB from January 2015 to December 2017 were reviewed till December 2020. The controls were matched with age, sex, and date of transplant. The first episode of GNB was taken. Clinical features, received anti-thymocyte globulin (ATG) or solumederol and cytomegalovirus infection (CMV) 90 days pre or post bacteremia, recurrent urinary tract infections (UTI), source of bacteremia and microbiology, all-cause mortality at day 28 and graft function at the last follow up were noted.
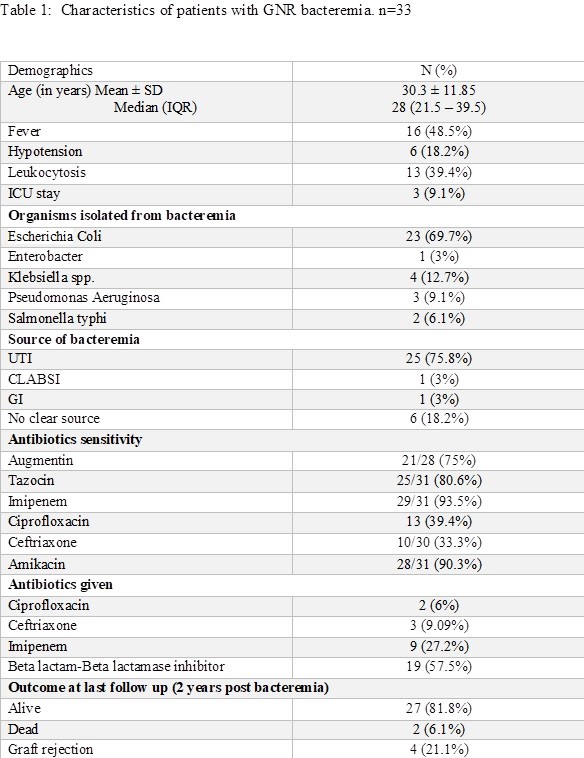
Results: Out of 1009 RTR, 33 (3.3%) episodes of GNB occurred. The mean age was 30±11.85years, 61% males. Around 48% developed bacteremia within 6 months post-transplant. The most common source was UTI (75.8%). Fever in 48% and only 39% had leukocytosis. Around 9% were admitted in the intensive care unit. E-coli was the most common organism (70%) (Table 1).
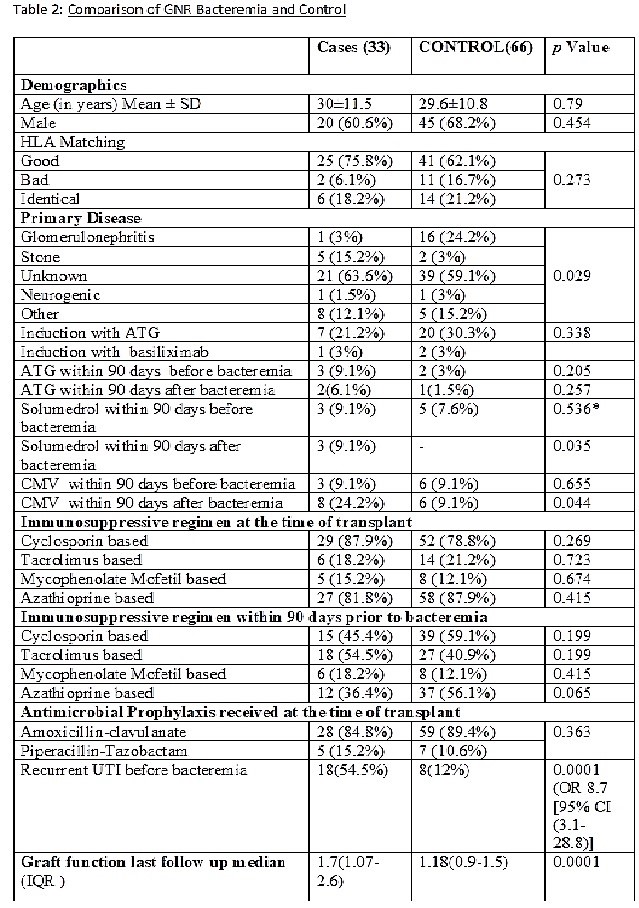
Stone disease at the time of transplant was significantly associated with bacteremia (p=0.029). There was no difference in receiving ATG or solumeredol and CMV before bacteremia. A significant number of patients received solumeredol for rejection (p=0.035) and had CMV (p=0.044) within 90 days after bacteremia. Recurrent UTI is significantly associated with bacteremia (p<0.001). The graft function at the last follow-up (2 years) was significantly deranged in patients with bacteremia (p=0.0001).
Conclusion: Gram-negative bacteremia was found in 3% of RTR and half of them developed within 6 months post-transplant. UTI was the most common source and recurrent UTI was significantly associated with bacteremia. The stone disease was the most significant risk factor. Patients develop rejection and CMV infection within 3 months post bacteremia. There was a significant graft dysfunction among patients with bacteremia at a mean follow-up of 2 years. We need to focus on the management of recurrent UTIs to prevent bacteremia and graft dysfunction in renal transplant recipients.

