
Is pregnancy possible in kidney transplant patients? Experience in a reference center in Mexico
Luis Garcia1,2, Karina Perez3, Flor Rojas3, Diana Fernandez1, Aldo Garcia1, Hector Hinojosa3, Lionel Vargas3.
1Surgery, Hospital General de Mexico Dr. Eduardo Liceaga, Ciudad de Mexico, , Mexico; 2Surgery, Hospital Especialidades CMN SXXI IMSS, Ciudad de Mexico, , Mexico; 3Nephrology, Hospital General de Mexico Dr. Eduardo Liceaga, Ciudad de Mexico, , Mexico
Background: The risk of complications during pregnancy is higher in women with CKD compared to healthy women, with a 10-fold increased risk for the development of preeclampsia, 5 times higher for the development of preterm labor and low birth weight, and 3 times the risk of termination of cesarean delivery. A recovery of fertility 6 months after transplantation has been observed in transplanted women.
Objective: To know the incidence of patients with pregnancy after kidney transplantation in our center, as well as the outcomes.
Methodology: A series of consecutive cases of post-transplanted women, over 18 years of age in our center from January 1, 2012 to January 1, 2020, who had at least one initial assessment at the time of pregnancy and a follow-up of at least 6 months, with adequate graft function at the time of pregnancy with adequate function of the graft at the time of pregnancy with its outcomes after the end of it. Data were collected retrospectively from their clinical record. Exclusion criteria: Patient with pregnancy prior to kidney transplantation, or whose follow-up is less than 6 months.
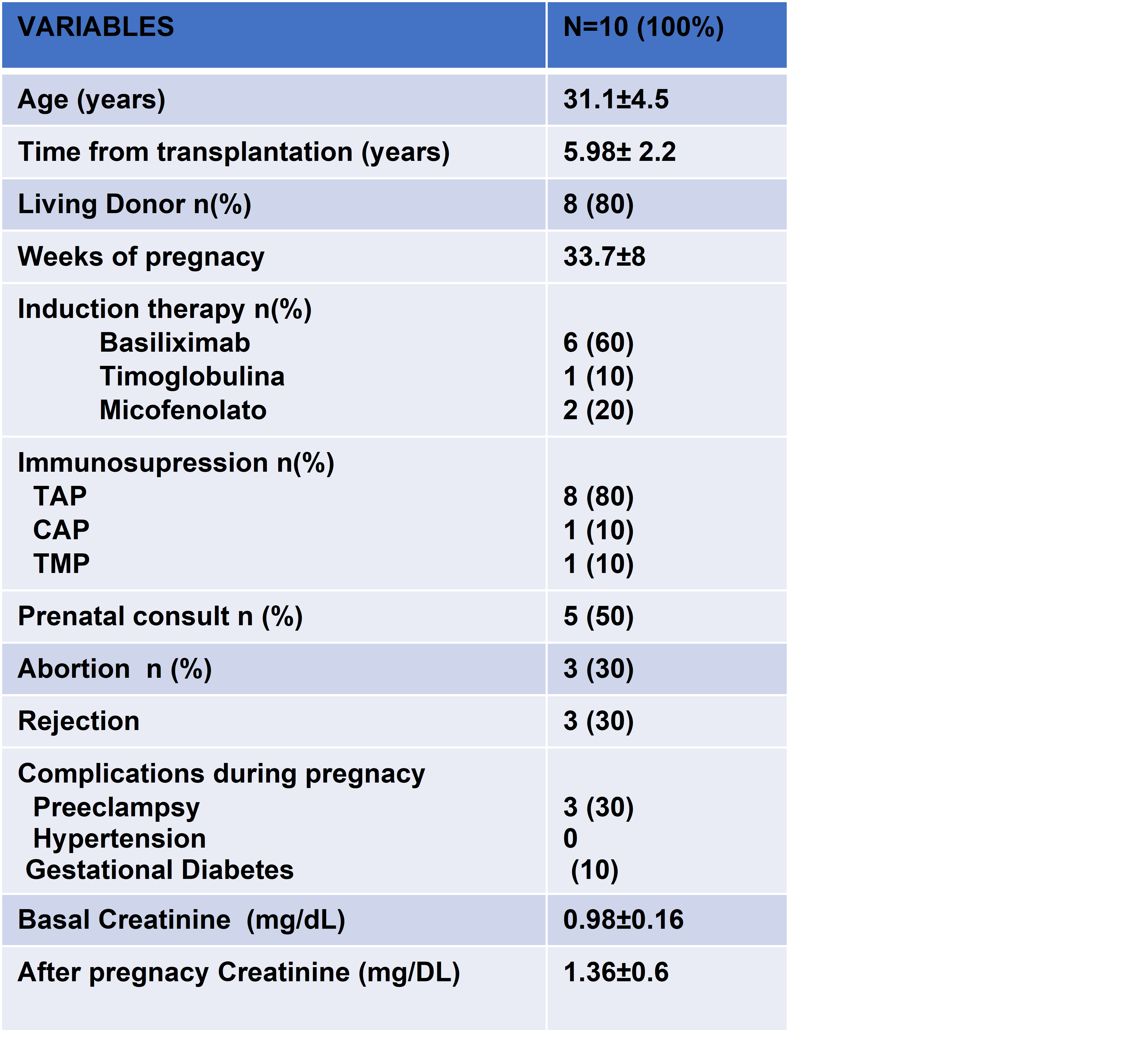
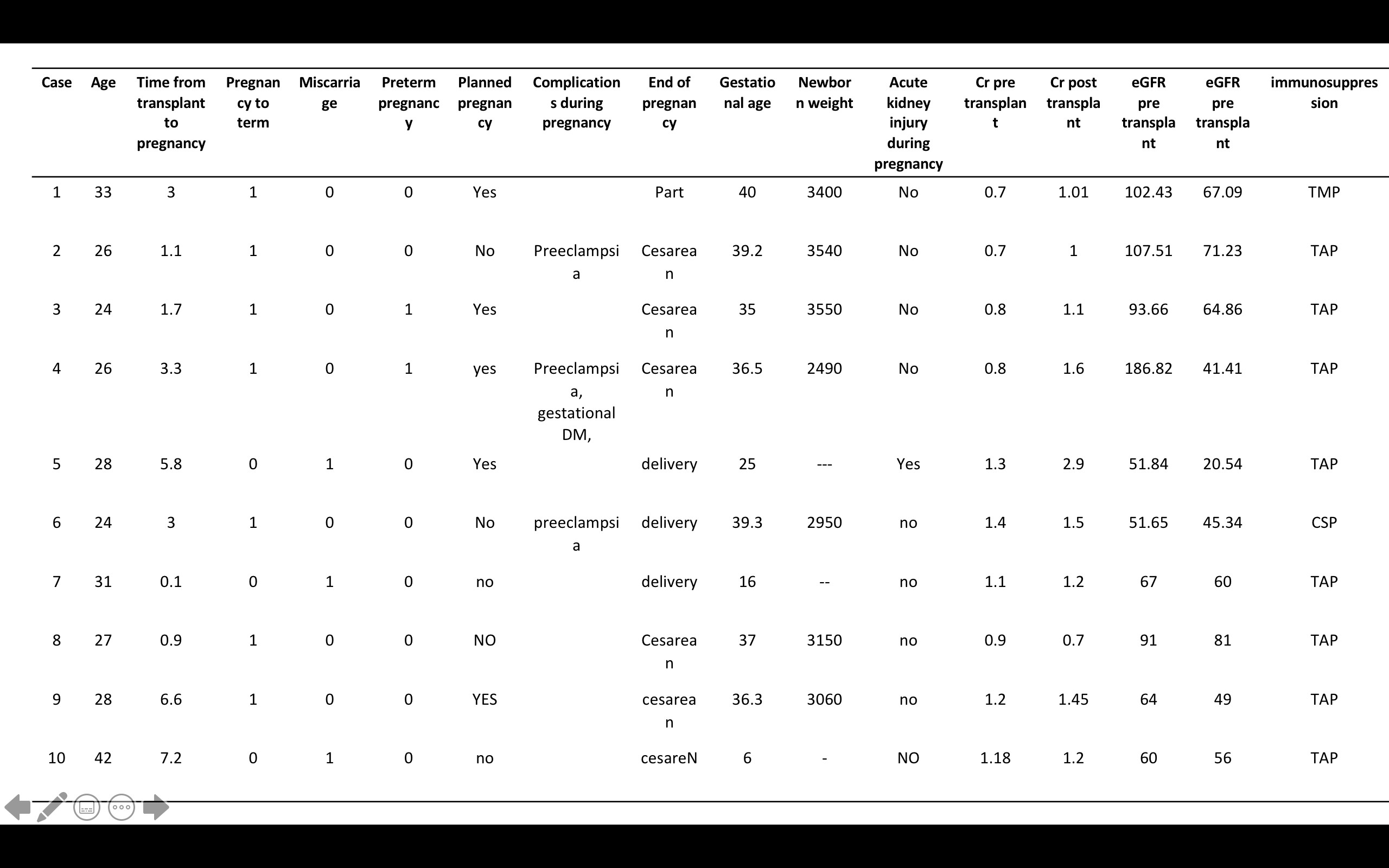
Results: We included 10 patients with chronic kidney disease and kidney transplantation, average age of 31.1±4.5 years, transplant interval of 5.98± 2.2 years, most received renal graft from a living donor, the main induction therapy was with Basiliximab.Maintenance therapy during pregnancy in 83.3% was modified to tacrolimus, azathioprine and prednisone, and in one patient presented with consumption of tacrolimus, mycophenolate and prednisone, which was one of the pregnant losses that occurred. 50% received prenatal consultation and pre-pregnancy counseling, considered as planned pregnancies; in 1 patient there was deterioration of renal function with graft dysfunction, without improvement after the end of pregnancy.
Discussion: Most women with kidney transplantation can carry a pregnancy to term with excellent results, although adverse events are common. Rates of preeclampsia, induction, and cesarean section were significantly higher compared to the general population. Most of the patients were able to be followed up for a period longer than 5 years, observing impairment of graft function in 40% of patients who presented pregnancy, 30% of these with return to renal function replacement therapy.
Conclusions: Pregnancy in transplant patients from our hospital does not differ from that reported in the literature; our cohort is limited, however it is considered of great importance to increase the number of studies of this however, it is considered of great importance to increase the number of studies of this type in our country and thus be able to improve strategies to obtain better maternal and fetal results throughout the post-transplant.

