
One OPO's experience with normothermic regional perfusion
Reid Freeman1, Heidi Wagenhauser1, Geoffrey Funk1, Douglas Butler1.
1Clinical Services, Southwest Transplant Alliance, Dallas, TX, United States
Introduction: The ability to increase the organ yield from Donation after Circulatory Death (DCD) donors is an urgent need. There have been advances in the ability to evaluate organs in a normothermic ex-vivo fashion, but the opportunity to perfuse and evaluate organs in-situ has been lacking. Normothermic Regional Perfusion (NRP) has provided transplant centers with the ability to assess organs on a DCD donor in similar fashion to the circumstances of Donation after Brain Death (DBD) procurement. This provides another option to increase the number of organs that are deemed suitable for transplantation.
Methods: We compared our traditional DCD donors (n=110) to our NRP DCD donors (n=9) from 1/01/2021-2/28/2022. We compiled data consisting of donor age, warm ischemic time (WIT), death pronouncement to NRP start, organs transplanted per donor, and recipient outcomes. From this data we determined averages and compared those to DCD recoveries completed without the use of NRP. We also compared recipient outcomes to DCD donors that utilized ex-vivo perfusion for the recovery and transplantation of the heart.
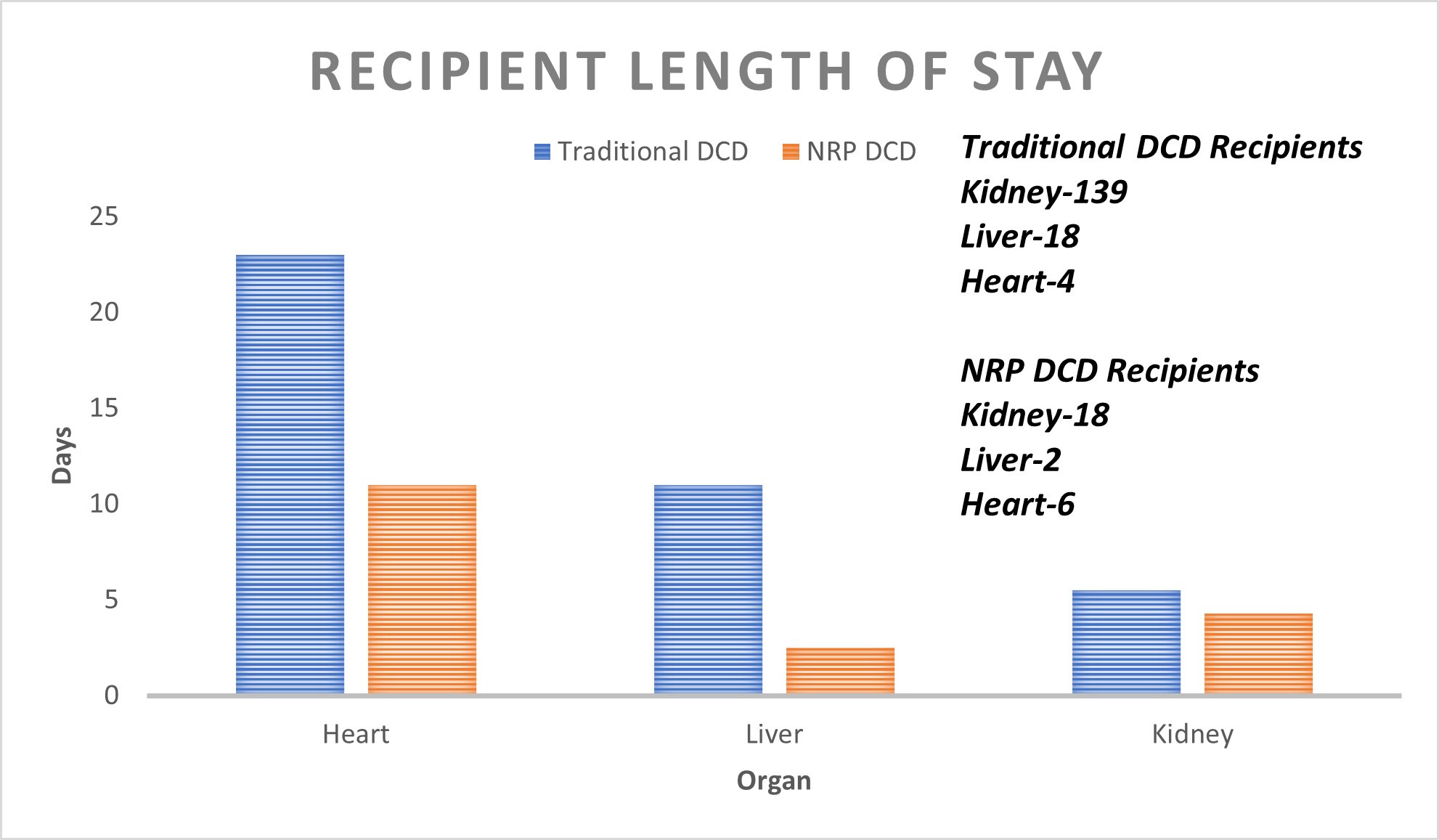
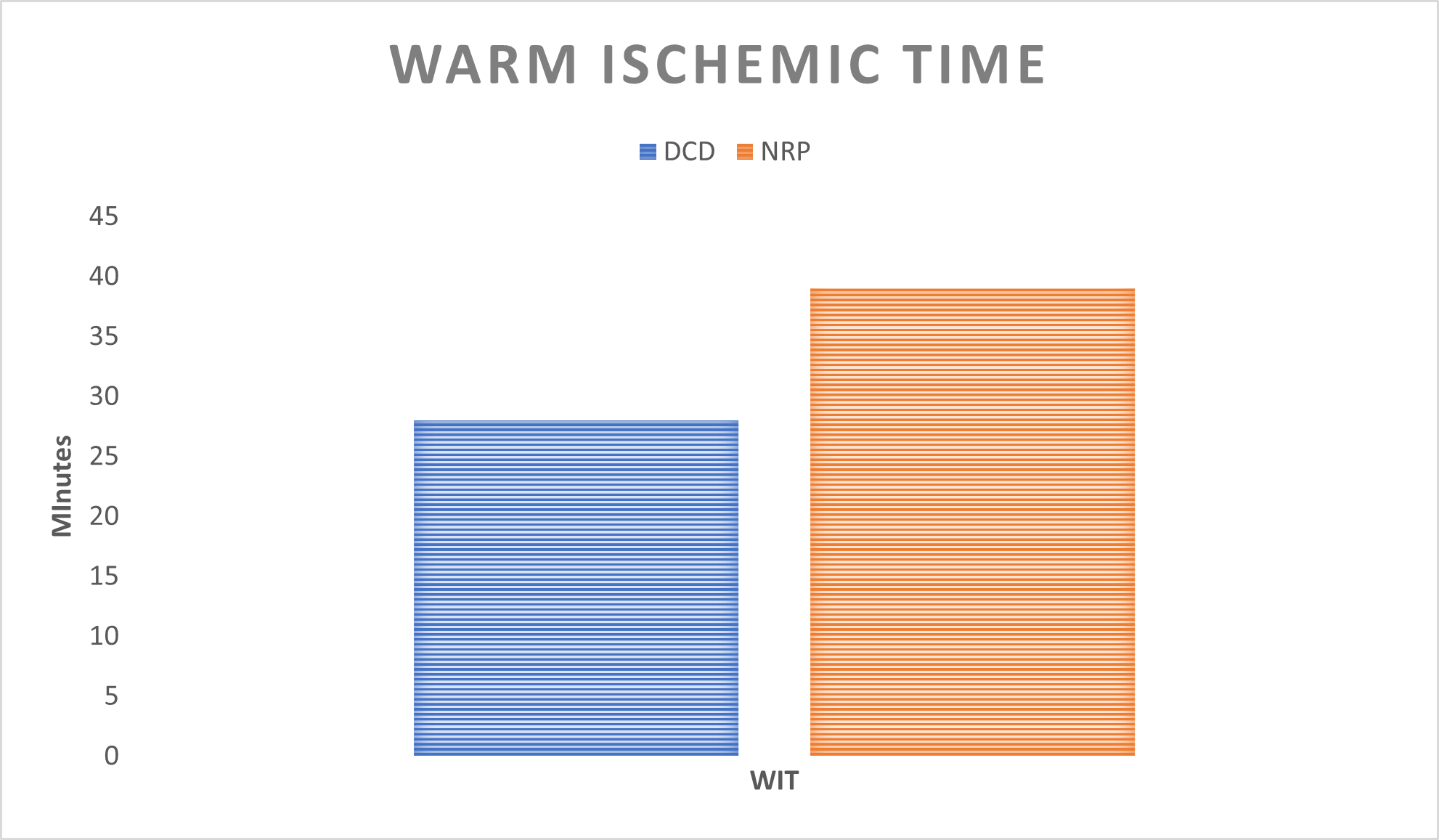
Results: Within our OPO, we define Warm Ischemic Time (WIT) as the start of the agonal phase (systolic BP < 80 mmHg or SpO2 < 80%) to NRP start. Warm ischemic time in NRP DCD patients includes both the agonal phase and time to initiation of artificial regional perfusion (averaging 7 minutes). Recipients from a DCD donor in which NRP was utilized had an average length of stay (LOS) of 6 days versus 13 days for traditional DCD. Compared to traditional DCD heart recoveries (average LOS 23 days with one patient expiring 42 days post-transplant), the NRP average length of stay was 11 days. NRP donors had a lower average age (33) to traditional DCD donors (49). Additionally, within the NRP DCD population, we saw a higher number of organs transplanted per donor (OTPD) by almost 1 organ with NRP DCD at 2.71 OTPD and traditional DCD at 1.88 OTPD. This is in spite of an increase in average WIT by 11 minutes for NRP donors.
Conclusion: NRP is a valid option for DCD recoveries and provides the accepting centers with an opportunity to evaluate the organs as they would in a DBD recovery. Utilizing NRP DCD allows for optimal utilization of donors which may in turn lead to acceptance of longer agonal phases and warm ischemic time if these results persist with larger study populations.

right-click to download