
Trends in kidney transplant usage after KAS implementation: is there evidence for a KDPI shift over time?
Molly Jacobs1, Robert Stratta1, Colleen Jay1.
1Surgery, Abdominal Organ Transplant, Atrium Health Wake Forest Baptist, Winston-Salem, NC, United States
Background: The Kidney Allocation System (KAS) was implemented in 2014, modifying allocation and introducing the Kidney Donor Profile Index (KDPI) as a metric of organ longevity and graft failure. KDPI >85% predicts a higher risk of graft failure, which may result in a negative labelling effect. High discard rates over time could engender a drift in the metric wherein “riskier” kidneys are not included in the pool and lower risk donors would then be associated with a higher score. We sought to determine transplant rates according to KDPI, changes in sharing according to KDPI, and characteristics of organs used in the pre and post KAS eras.
Methods: Using UNOS data, we compared overall, local, regional, and national utilization for deceased donor kidney transplants (DDKT) alone according to KDPI group and KAS era: Era 1 (2010-2011, pre-KDPI), Era 2 (2012-2013, pre-KAS), Era 3 (2014-2015, early post-KAS), Era 4 (2016-2017), and Era 5 (2018-2020).
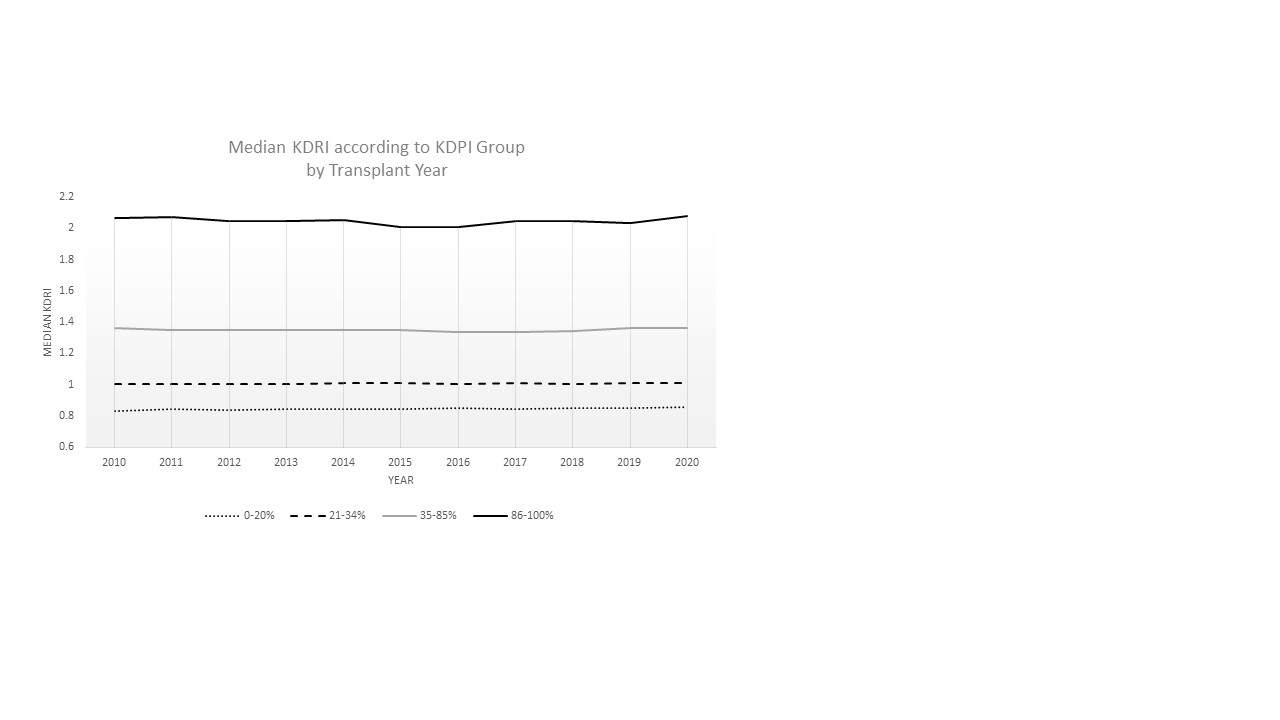
Results: Despite an initial decline in the average KDPI utilized after implementation of KAS for allocation in Era 3, a rebound occurred, resulting in an overall higher average KDPI used for transplant in Era 5 than pre-KAS (p<0.01). KDPI >85% usage similarly declined from Era 1-4, with recovery in Era 5 (p<0.01). Donor age >60, diabetes, and hypertension showed similar declines early post-KAS with recovery in the final era. The proportion of DCD donors, HCV Ab and NAT positivity, and elevated donor terminal creatinine increased in each subsequent era. Overall, there were no significant differences in median KDRI according to KDPI group from 2010 to 2020 to suggest a “KDPI drift” (See Figure 1). Since KAS, sharing increased across all KDPI groups, but was more pronounced with increasing KDPI.
Conclusion: After initial dips in utilization of high KDPI organs after KAS implementation, trends reversed with higher mean KDPI and proportion of KDPI>85% utilization in the most recent era. Growth in utilization of DCD and HCV (Ab+ and NAT+) organs has occurred over time. Overall, we did not find evidence for a shift to increasingly risk-averse practices according to KDPI following KAS, and changes in regional utilization suggest better direction of these organs to programs willing to utilize them. Further changes are still need to achieve the goal of significantly reducing discard rates for high KDPI organs.

right-click to download