

Treatment of complex desmoid tumours by intestinal transplantation
Emilio Canovai1,2, Andrew Butler1,2, Charlotte Rutter1,3, Lisa Sharkey1,3, Dunecan Massey1,3, Jeremy Woodward1,3, Neil Russell1,2, Irum Amin1,2.
1Cambridge Centre for Intestinal Rehabilitation and Transplant (CamCIRT), Addenbrooke's Hospital, Cambridge, United Kingdom; 2Department of Transplant Surgery, Addenbrooke's Hospital, Cambridge, United Kingdom; 3Department of Gastroenterology, Addenbrooke's Hospital, Cambridge, United Kingdom
Introduction: Desmoid tumours are rare, locally aggressive tumours which often have an unpredictable and variable clinical course. Although most desmoids (80%) are sporadic, 20% are associated with Familial Adenomatous Polyposis (FAP) which tend to be multi-focal and more aggressive. While the majority of desmoids can be managed by watchful waiting, systemic therapy or radiotherapy, some will require surgical excision. It is recommended in these cases to perform a total resection to reduce the chance of recurrence. In the most extreme cases (multiple segments of bowel, complex fistulating disease, invasion into the abdominal wall, ureteric encasement), the most radical option is to perform a total enterectomy and Intestinal Transplant (ITx). The decision if and when to refer a desmoid patient for ITx can be challenging, particularly the timing and sequence of treatment (simultaneous vs sequential exenteration + delayed listing for ITx). In this study, we present our centre’s experience of managing complex, desmoid tumours with ITx.
Method: We performed a retrospective case review of our prospectively collected database between 2007 and 2022. All patients receiving an ITx for desmoids were identified.
Results: Between 10/2007 and 03/2022, 126 ITx in 119 patients were performed at our centre. Of these, 14 patients (12%) were for desmoid disease (6 Modified Multivisceral Transplants (MMVT), 5 Isolated ITx and 3 Liver-Small bowel Transplant. Median follow was 43 months (7-104). 9 out of 14 patients are alive (64%) without GI recurrence. None of the patients died from desmoid recurrence. The management of this cohort presented us with several complex technical issues that needed to be overcome such as loss of abdominal domain (6/14), retroperitoneal involvement (6/14), pouch related issues (2/14) and the need for a gastrectomy/duodenectomy due to dysplastic disease (6/14). Loss of abdominal domain and invasion/destruction by the desmoid disease was addressed by using non-vascularised rectus fascia (NVRF), either on its own (4/6) or in combination of vascularized muscle flaps (2/6).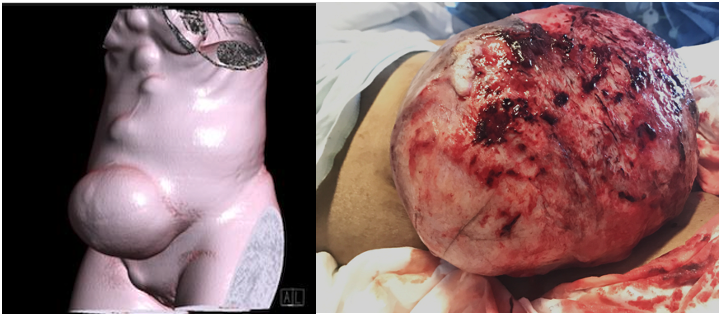

Retroperitoneal involvement of the vena cava/iliac vessels and the ureters. Two of these patients required a renal auto-transplantation into the iliac fossa while one patient had a ureteric re-implantation from right to left. The decision to also remove stomach and/or duodenum at the time of ITx depends on the risk of polyp malignancy. Pre-operative polyp surveillance, histology and the Spiegleman score help us to determine the need for a MMVT.
Conclusion: Intestinal Transplantation is a viable treatment option in selected patients with extensive desmoid disease. Deciding which patients would benefit from ITx is important to ensure timely referral. Delays in this process can result in additional disease burden such as secondary liver disease or invasion of adjacent structures, requiring further reconstructions.

right-click to download