
Impact of left ventricular ejection fraction and previous cardiac revascularization on patient and graft survival in kidney transplant receipts
Dominic Amara1,2, Miguel Nunez2, Justin Parekh3, David Foley4, Stuart Greenstein5, Ryutaro Hirose6.
1Department of Surgery, University of California, Los Angeles, Los Angeles, CA, United States; 2School of Medicine, University of California, San Francisco, San Francisco, CA, United States; 3Department of Surgery, University of California, San Diego, San Diego, CA, United States; 4Department of Surgery, University of Wisconsin, Madison, WI, United States; 5Department of Surgery, Montefiore Medical Center, Bronx, NY, United States; 6Department of Surgery, University of California, San Francisco, San Francisco, CA, United States
Background: Single center studies have implicated baseline left ventricular ejection fraction (LVEF) and baseline coronary artery disease as strongly associated with post-kidney transplant graft and patient survival, including in limited multivariate models. However, the United States’ Scientific Registry of Transplant Recipients (SRTR) does not directly include any cardiac variables as part of its risk adjustment model, raising the question of whether the current SRTR model fairly risk adjusts potential recipients.
Methods: This study used the novel prospective United States National Surgical Quality Improvement Program (NSQIP) Transplant database to assess the impact of LVEF and pre-transplant revascularization on post-transplant outcomes in deceased donor renal transplantation (DDRT). Recipients from 2017-2019 were identified and stratified by LVEF into <50 and 50+ categories. A separate analysis stratified patients into if they had received pre-transplant revascularization, defined as either coronary bypass surgery or percutaneous intervention. Post-transplant outcomes were assessed.
Results: A total of 2377 DDRT recipients were included from 29 centers. Mean follow up was 200 days. Only 4.8% had LVEF<50 at transplant, while 13.3% had undergone cardiac revascularization prior to transplant. There were several baseline differences between patients who did and did not have previous revascularization.
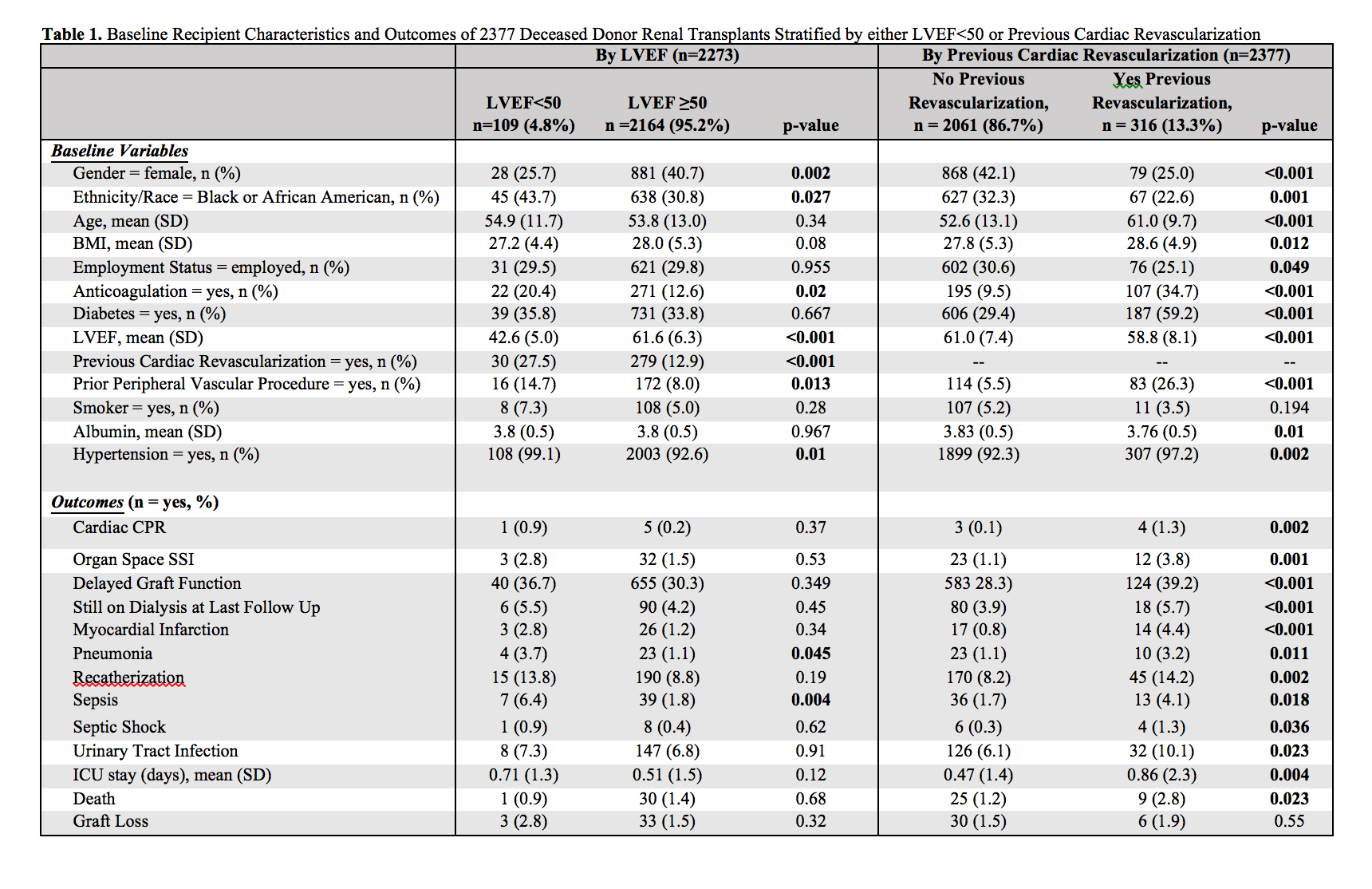
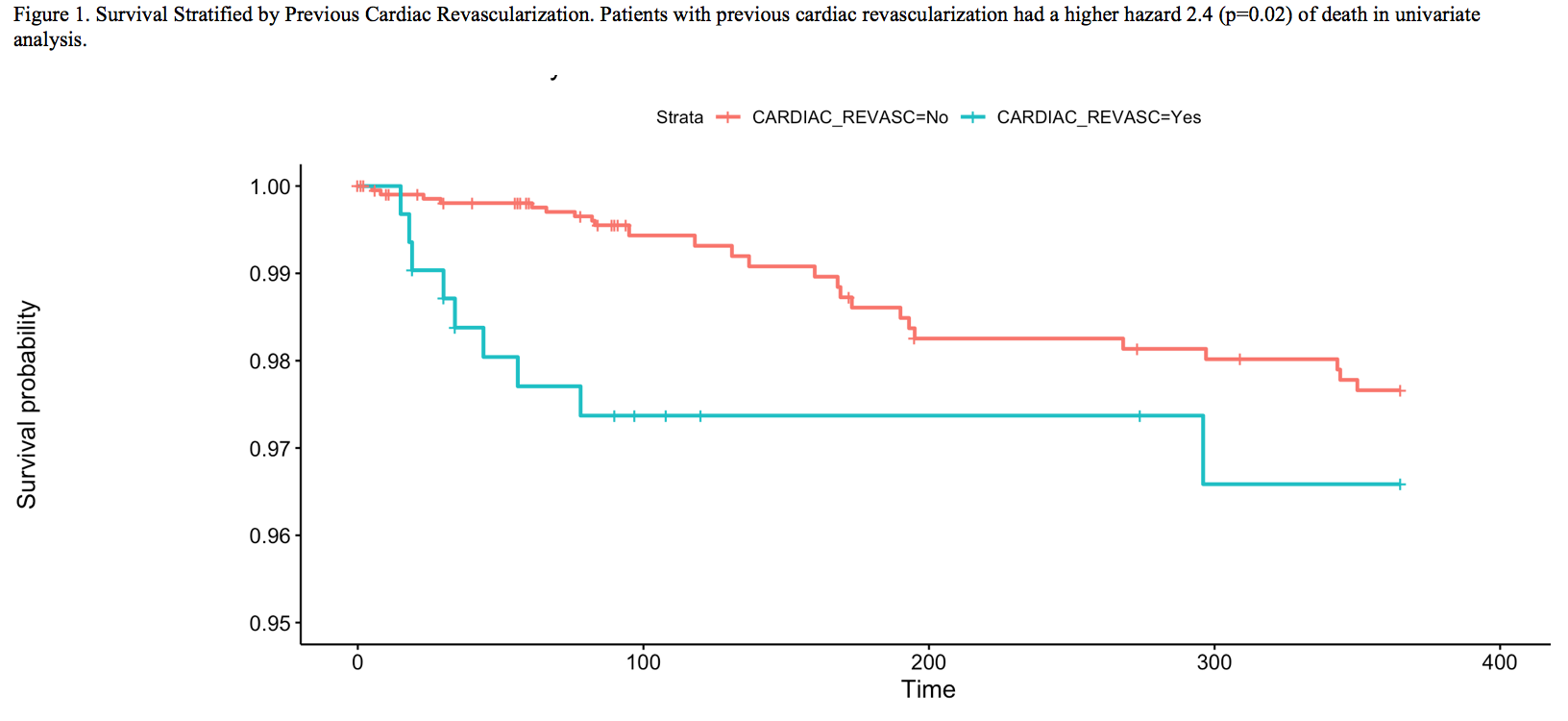
Previous revascularization was associated with increased risk of requiring cardiac CPR (1.3 vs 0.1%, p=0.002), organ space surgical site infection (3.8 vs 1.1%, p=-0.001), delayed graft function (39.2 vs 28.3%, p<0.001), requiring dialysis at last follow up (5.7 vs 3.9%, p<0.001), myocardial infarction (4.4 vs 0.8%, p<0.001), pneumonia (3.2 vs 1.1%, p=0.011), recatherization (14.2 vs 8.2%, p=0.002), sepsis (4.1 vs 1.7%, p=0.018), septic shock (1.3 vs 0.3%, p=0.036), UTI (10.1 vs 6.1%, p=0.023), and longer ICU stay (0.86 vs 0.47 days, p=0.004). In univariate analysis, previous revascularization was associated with increased hazard of death (HR 2.4, p=0.02) but not graft loss (HR 1.3, p=0.52). In a multivariate model including previous revascularization and existing SRTR variables (age, diabetes, peripheral vascular disease, albumin, KDRI) as predictors, previous revascularization was related to a higher hazard of death (HR 1.43) however this was not a statistically significant finding (p=0.42).
Conclusions: We conclude that in the DDRT in patients with previous cardiac revascularization is much more common (13.3%) than in those with LVEF<50 (4.8%). We also demonstrate that previous cardiac revascularization is a powerful predictor of both patient survival and several post-transplant complications. However, we also show that existing variables (e.g. diabetes, PVD, age) in the SRTR risk stratification model largely capture the impact of previous cardiac revascularization on patient survival at least in the early follow up period.

right-click to download