
Save the environment: liver transplantation restores a circulating environment that supports healthy platelet aggregation within two hours of reperfusion
Hillary Braun1, Alex T Fields1, Kim Rodriguez1, Zachary A Matthay1, Rishi Kothari2, Claus U Niemann2, Dieter Adelmann2, Nancy L Ascher1, John P Roberts1, Michael P Bokoch2, Lucy Z Kornblith1.
1Surgery, University of California, San Francisco, San Francisco, CA, United States; 2Anesthesia, University of California, San Francisco, San Francisco, CA, United States
Introduction: Thrombocytopenia in patients with cirrhosis is common and likely multifactorial secondary to splenic sequestration, decreased thrombopoietin production, shear stress of portal hypertension, and toxic suppression of megakaryocytopoiesis. However, there is no clear association of absolute platelet count with risk of hemorrhage. Rather, platelet dysfunction, in the pro-inflammatory vasodilatory state of chronic liver disease, may be of greater importance. There is evidence that the circulating environment of severe tissue injury and shock impairs platelet aggregation in trauma patients. Using this model as our template, we hypothesized that healthy platelets treated with serum from cirrhotic patients pre-transplant would have impaired aggregation compared to those treated with serum post-portal reperfusion.
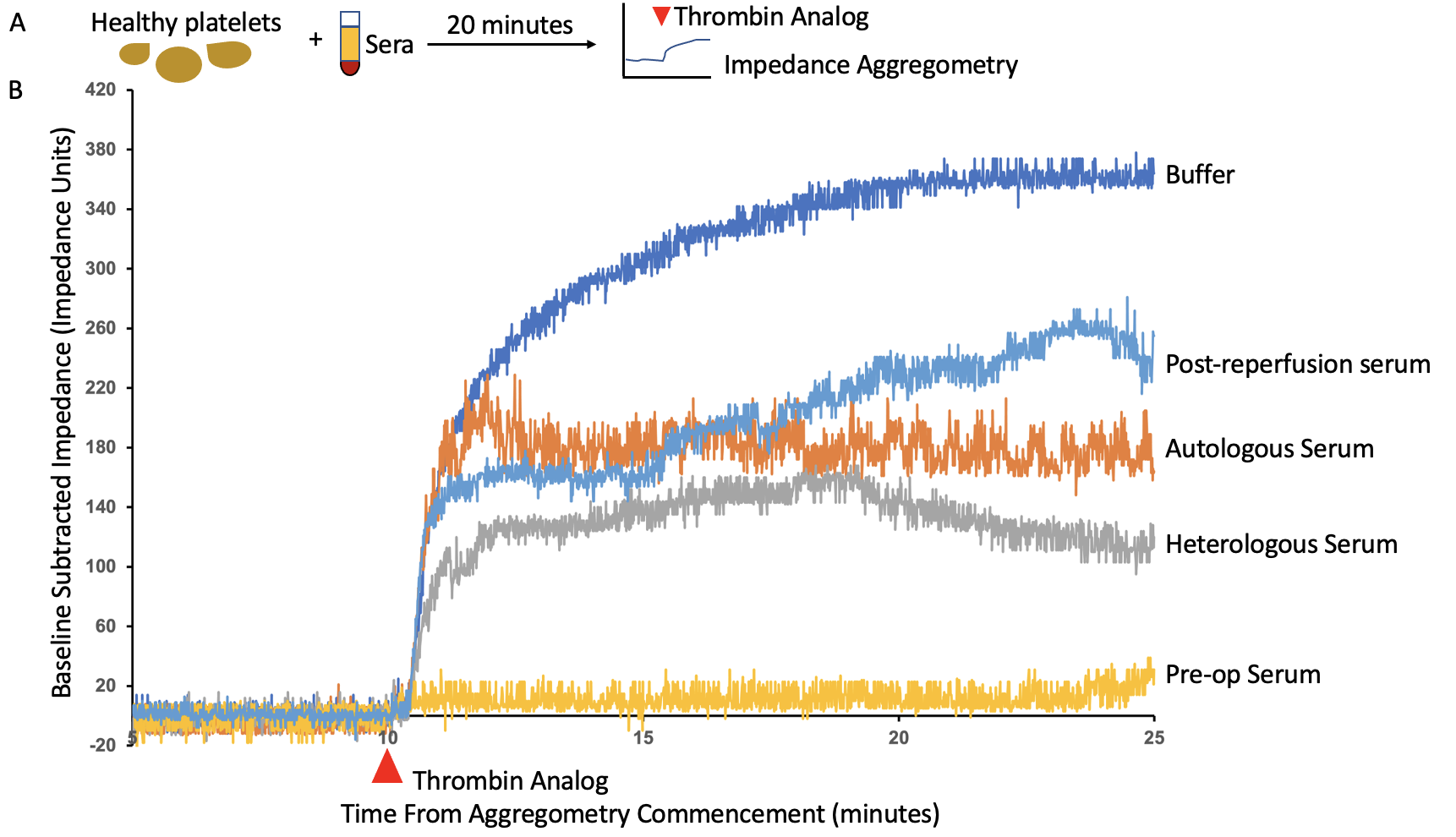
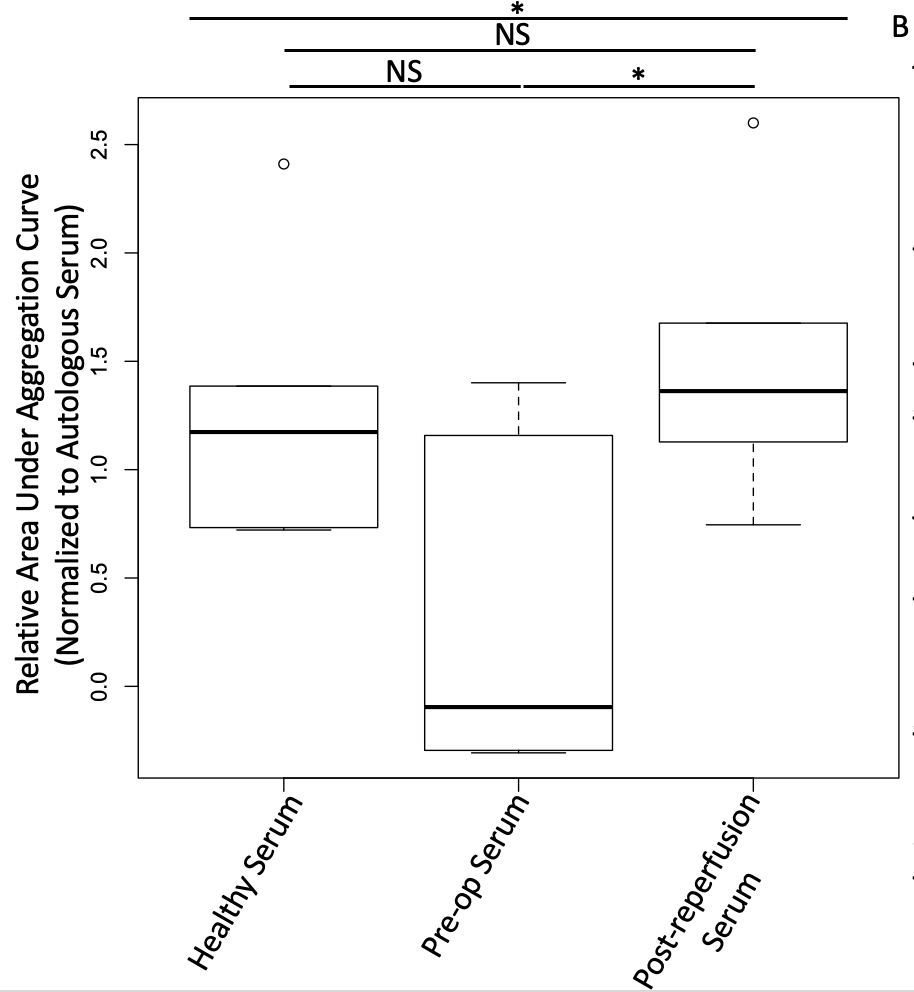
Methods: Serum was collected from liver transplant recipients prior to incision, and two hours following portal reperfusion as part of the Mild Hypothermia and Acute Kidney Injury in Liver Transplantation trial (NCT03534141). Platelets (from male and female healthy platelet donors) were isolated by centrifugation, pelleted, and mixed with each of the following sera (6 of each group): buffer, autologous, gender matched healthy (heterologous), gender matched pre-transplant, and gender matched post-portal reperfusion (12% v/v) for 20min (Fig1A). Baseline aggregation was measured for 10min via multiple impedance aggregometer, then stimulated with a thrombin analog and measured for 15min. Aggregometry responses were quantified by the area under the impedance aggregation curve (AUC), normalized to autologous treated platelets. Statistical analysis was performed using one way ANOVA, with Tukey’s Honest Significant Difference testing post-hoc for pairwise comparisons.
Results: Healthy platelet aggregation was markedly impaired upon treatment with pre-transplant serum, but was restored when treated with serum from the same cohort of patients two hours post-portal reperfusion (to levels similar to treatment with healthy sera, Fig1B). Healthy platelet aggregation upon treatment with post-portal reperfusion serum was significantly higher than with pre-transplant serum treatment (median relative AUC 1.4x vs -0.1x, p<0.05; Fig2).
Conclusion: Healthy platelets treated with serum from cirrhotic patients immediately prior to liver transplant have impaired aggregation, while treatment with serum from the same patients two hours post-portal reperfusion restores aggregation. This suggests the circulating environment of cirrhosis may induce platelet dysfunction through soluble inhibitors, and that liver transplantation and the healthy plasma administration accompanying the reperfusion phase, may induce swift recovery of platelet aggregation capacity. Future investigations should focus on implications of this including that platelet transfusion may not achieve hemostasis until post portal-reperfusion.

right-click to download