
Salvaging small for size grafts with splenic artery embolization in living donor liver transplant: older liver may not recover
Sorabh Kapoor1,2, Rozil Gandhi3, Pathik Parikh5, Gaurav Goswami4, Vibha Varma1,6.
1Liver Transplant & HPB Surgery, Zydus hospital, Ahmedabad, India; 2Abdominal Transplantation, UNC Health, CHAPEL HILL, NC, United States; 3Interventional Radiology, Zydus hospital, Ahmedabad, India; 4Radiodiagnosis, Zydus hospital, Ahmedabad, India; 5Hepatology, Zydus hospital, Ahmedabad, India; 6Liver Transplant & HPB Surgery, Max Hospital, New Delhi, India
Introduction: Small for size (SFS) is a dreaded problem after LDLT. Portal hyperfperfusion (large spleen) or outflow issues can cause functional SFS despite adequate GRWR (> 0.8). SAE (Splenic Artery Embolization) reduces portal flow allowing the graft to recover and regenerate. However,despite SAE, older grafts may not recover from the hyperperfusion injury. We report 3 cases which required SAE and discuss the outcomes.
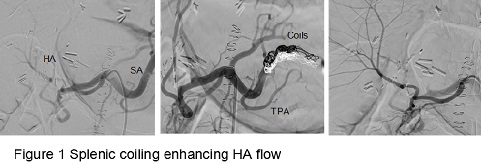
Method: Medical records of 3 male patients with right lobe LDLT (donors - spouses) who underwent SAE with a diagnosis of SFS were reviewed. Median MELD was 25 and donor age were 39, 40 and 59 years. Two presented with functional SFS; GRWR 0.83 and 0.82 (RIHV thrombosis leading to hyperperfusion); 1 patient (hyperperfusion due to enlarged spleen;GRWR 0.89) also had Splenic arterial steal on Doppler (patent artery on CT angiography). All 3 had initial reduction of bilirubin and INR till POD4 followed by worsening LFT and ascites.SAE was done after Doppler findings /Triphasic CT /MRI and no suspicion of biliary issues.{{AbstractFigure.1}
Results: SAE was successful in reducing portal flow in all 3.The patients with younger grafts(Donor age<45 )showed rapid improvement; normalization of bilirubin and disappearance of ascites over next 2 weeks. However, the patient with older graft after showing initial reduction of bilirubin and ascites (Doppler showed continuous >30 % reduced portal flow) had worsening jaundice,ascites, coagulopathy and hypoalbuminemia. He subsequently developed severe graft dysfunction and septicemia and expired.
Conclusion: SFS can manifest despite adequate GRWR(>0.8), if outflow issues / hyperperfusion are present. SAE works well in salvaging SFS post operatively, but older livers may not have enough reserve to recover. When accepting older livers, intra op flow and pressure recording may be used to perform Splenic artery ligation or Splenectomy to prevent SFS.

right-click to download