
Renal transplantation and statins effects on dyslipidemia in renal transplant recipients
Ziad Arabi1,2,3, Abdullah Alghamdi1,2,3, Ahmad Alnasrullah1,2,3, Mohammed Tawhari1,2,3.
1Division of Nephrology, Department of Medicine, King Abdulaziz Medical City, Riyadh, Saudi Arabia; 2King Abdullah International Medical Research Center, Riyadh, Saudi Arabia; 3College of Medicine, King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia
Purpose: To review the effect of renal transplantation and adding of statins on dyslipidemia in renal transplant recipients.
Methods: A single center experience retrospective study of renal transplant recipients, from 2017 to 2020. Lipids' profile and Hgb A1C were reviewed at baseline (before transplant) and at average12 months follow-up of renal transplant recipients who received statins or not.
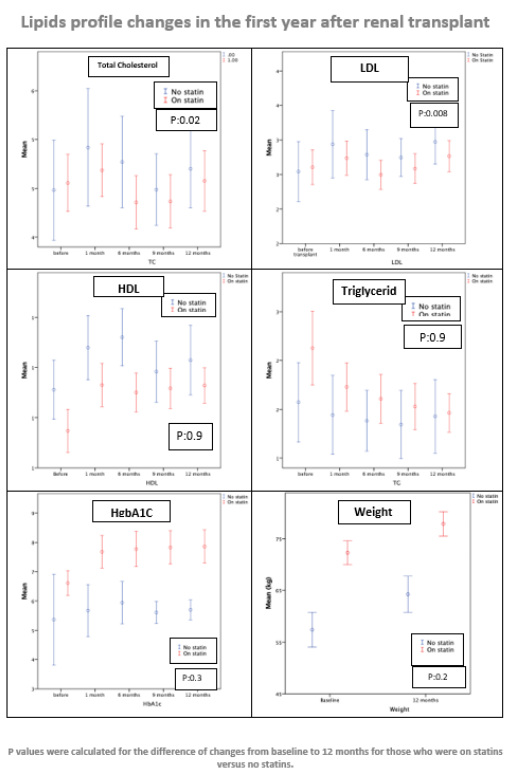
Results: 287 renal transplant recipients were included. 74% were ≥ 30 years, men: 58% and living-donor kidney recipients: 80%. Statins were prescribed to 80% of kidney recipients who were ≥30 years old and to 33% who were <30 years old. 28% of the recipients were already on statins before the renal transplantation. Whereas statins were initiated in 26% before discharge from the transplant admission, or during the first year in 14%. While 32% did not receive any statins. The most common statin used was Atorvastatin at 10 mg in 60% or 20 mg in 23% of the cases. In patients who did not receive statins: renal transplantation was associated with a significant increase of total cholesterol (TC) by 0.31 mmol /L (0.04 to 0.59: P: 0.026) and a significant increase of LDL by 0.40 mmol /L (0.16 to 0.65; P:0.001). On the other hand, and despite weight gain of average 6.9 kg ( P <0.001), and increased AIC by 0.71(P<0.001); renal transplantation was associated with an increase of HDL by 0.17 mmol /L (0.09 to 0.25; P:<0.001) and down trending but not statically significant decrease of triglyceride (TG) by -0.09 mmol /L (-0.25 to 0.07; P: 0.280). In renal transplant recipients who received statins: despite weight gain of 5.6 kg (P:<0.001) and increased A1C by 0.93 (P: <0.001), HDL improved by 0.17 mmol /L (0.13 to 0.22; P<0.001) and TG decreased by -0.34 mmol /L (-0.50 to -0.17; P:<0.001). Statins were associated with a numerical decrease of TC by -0.06 mmol /L (-0.23 to 0.12; P: 0.519) and nonsignificant increase of LDL by only 0.04 (-0.10 to 0.18, P: 0.607). Statins were significantly associated with improvement of TC and LDL compared to no statins. The mean changes of TC (from baseline to 12 months) while on stains versus none were (-0.06 mmol /L ±1.16 versus 0.31 mmol /L ±1.12; P: 0.026) and the mean changes of LDL while on stains versus none were (0.04 mmol /L ±0.96 versus 0.40 mmol /L ±1.02; P: 0.008).
Conclusions: Despite weight gain and the increased level of A1C seen after renal transplantation, renal transplantation was associated with improved TG and HDL. Adding statins in patients at higher risk of dyslipidemia not only maintained the beneficial effects of renal transplantation on HDL and TG but also had significant “buffering” effect against the rising of TC and LDL.

right-click to download