
Protective effect of HLA-A24 allele on COVID-19 among vaccinated kidney transplant recipients
Natsuki Eguchi1, Ekamol Tantisattamo2, Uttam Reddy2, Antoney Ferrey2, Donald Dafoe1, Hirohito Ichii1.
1Surgery, University of California Irvine, Orange, CA, United States; 2Medicine , University of California Irvine, Orange, CA, United States
Introduction: Human Leukocyte Antigen (HLA) alleles have been shown to affect both the susceptibility and severity of viral infections. [1] Recently, seasonal coronavirus-specific CD8+ T cells were found to cross-react with HLA-A24 high binding epitope from SARS-COV2 spike protein in healthy persons with HLA A-24 alleles. [2] Considering that HLA-A24 antigen has been found in high frequency in Asian countries that have experienced the lowest death per capita, HLA-A24 allele may confer protection against COVID 19. Therefore, in this study, we examined the association of HLA-A24 allele and COVID19 susceptibility and severity in kidney transplant recipients (KTR).
Methods: A single-center cross-sectional study included 530 patients who received a kidney transplant between 2/1/2017 to 1/31/2022. The exposure was HLA-A24 allele and primary outcomes were COVID19 infection and COVID-19-related hospitalization or COVID-19-associated death. All positive COVID-19 KTR were either self-reported or were from PCR tests indicated for patients with COVID-19 symptoms. For further analysis, patients were stratified by vaccination status prior to COVID-19 infection. Data was analyzed using student's T test, Chi square test, and Fischer exact test.
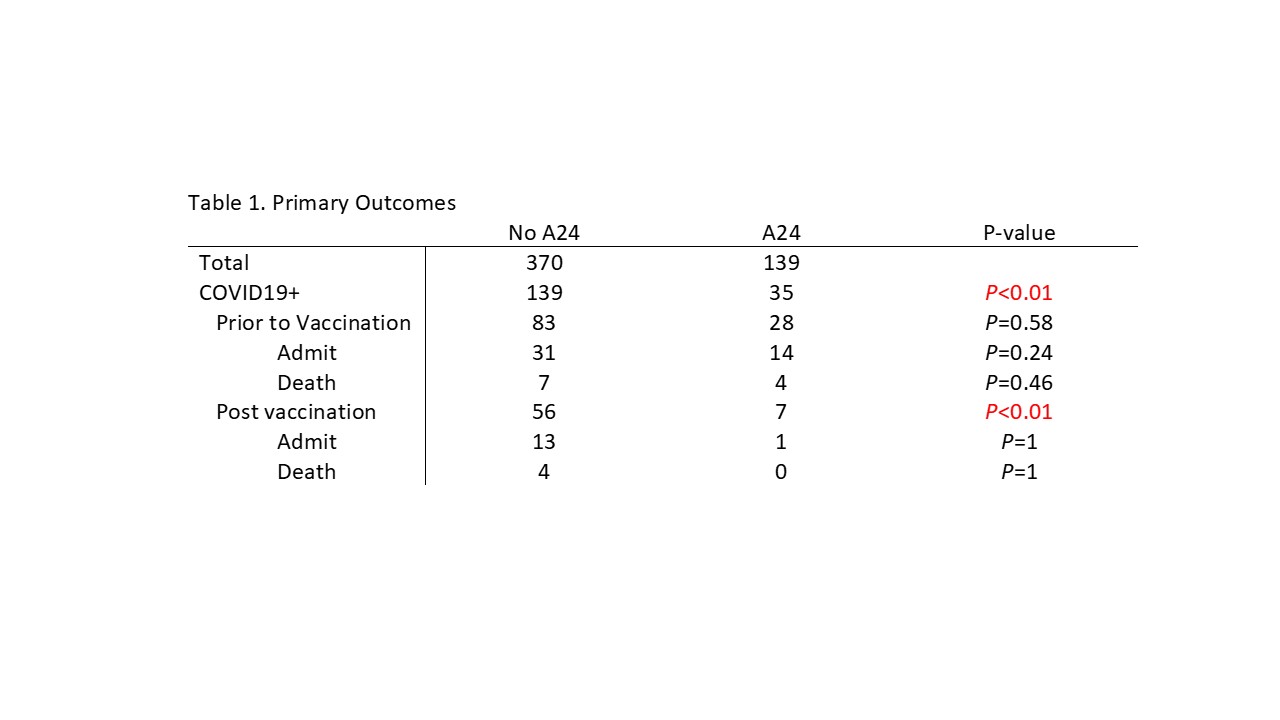
Results: Of the 509 KTR, 139 (27%) patients had at least one HLA-A24 antigen of which 13 patients were double-positive for HLA-A24. There were no significant differences in age, gender, race, ethnicity, BMI, and prevalence of comorbidities including coronary artery disease, diabetes, and heart failure between patients with and without HLA-A24 allele. Of 139 KTR with HLA-A24 alleles, 35 patients became infected with COVID-19; while 139 of 370 KTR without HLA-A24 had COVID-19 (25.2% vs. 37.5%; P <0.01). After stratified by vaccination status prior to COVID-19 infection, while the ratio of KTR with COVID-19 prior to vaccination did not differ between the two groups (20.1% vs. 22.4%, P =0.58), the proportion of patients who had COVID-19 after vaccination was significantly lower in the HLA-A24 group (5.0% vs. 15.1%; P <0.01). There was no difference in hospitalization and mortality related to COVID-19 between the two groups.
Conclusion: COVID-19 vaccination is more effective in KTR with HLA-A24allele. Further studies are required to elucidate the mechanism of protective effect of HLA-A24 on COVID-19 in high-risk immunocompromised host such as in KTR.
References:

