Donor hypertension is associated with an increased risk of early pancreas allograft failure
Christophe Masset1,2, Julien Branchereau2,3, Florent Leborgne5, Lionel Badet4, Christophe Legendre6, Gilles Blancho1,2, Magali Giral1,2, Georges Karam3, Jacques Dantal1,2, Diego Cantarovich1.
1Service de Néphrologie et Immunologie Clinique, Institut de Transplantation Urologie Néphrologie , Nantes, France; 2Center for Research in Transplantation and Translational Immunology, UMR 1064, Université de Nantes, Nantes, France; 3Service d'urologie, Institut de Transplantation Urologie Néphrologie , Nantes, France; 4Service d'urologie chirurgie de la transplantation, Groupement Hospitalier Edouard Herriot , Lyon, France; 5INSERM UMR 1246 - SPHERE, Université de Nantes, Nantes, France; 6Department of Nephrology and Kidney Transplantation, Necker Hospital, Assistance Publique-Hôpitaux de Paris, Paris, France
DIVAT Pancreas Consortium.
Background: About 10% of pancreas allografts are still lost prematurely, despite identification of numerous thrombosis risk factors. We investigated for potential other undescribed risk factors for early pancreas failure.
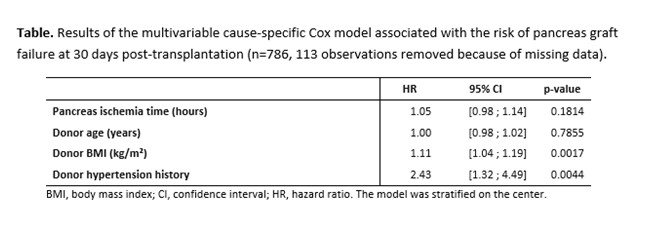
Methods: We conducted a multicentric study including 899 pancreas transplantations between 2000 and 2018. Early pancreas failure, long term pancreas survival, kidney and patient survival were analyzed depending on multiple donor, recipient and perioperative transplantation characteristics using a multivariable cause-specific Cox models stratified on transplant centers.
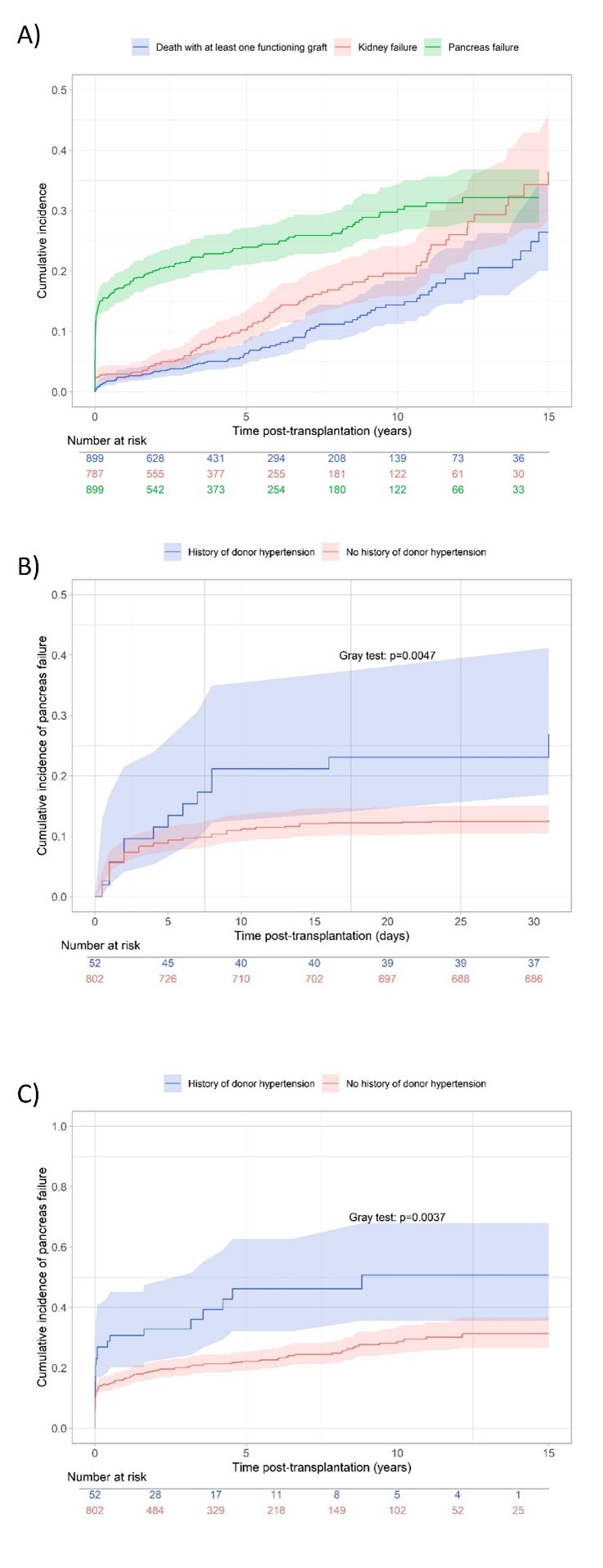
Results: Donor hypertension and donor BMI were significatively associated with an increased risk of early pancreas lost (respectively : HR = 2.43, 95% CI from 1.32 to 4.49 and HR = 1.38, 95% CI from 1.13 to 1.68) and thus of impaired long-term pancreas survival (HR = 1.88, 95% CI from 1.13 to 3.12 and HR = 1.21, 95% CI from 1.04 to 1.41 respectively). However, donor hypertension had no impact on pancreas allograft survival since day 30 post-transplantation (respectively, HR = 1.22, 95% CI from 0.47 to 3.15), neither on kidney allograft survival (HR = 1.58, 95% CI from 0.80 to 3.10 p = 0.1844). Donor hypertension was uncommon (5.7% of donors) but associated with an increased risk of allograft failure compared to non-hypertensive donors: 12.6% vs 26.9% at one month; 28.8% vs 50.7% at 10 years, p = 0.0037.
Conclusion: Despite rare, pancreas transplantation from hypertensive donors is associated with an increased risk of early pancreatic allograft failure, without significant effect on kidney allograft function, suggesting different pathophysiological mechanisms that the ones commonly described as atherosclerosis.