

Cryopreserved vs non-cryopreserved graft before autologous stem cell transplantation in patients with multiple myeloma. A comparative study
Leandro Castellanos1, Pablo Garcia M.D1, Maria Teresa Oliva1, Vanina Acosta3, Cosntanza Bianchi3, Norma Escalante1, Claudia Rosi1, Mercedes Garcia M.D1, Gabriela Sturich M.D1, Juan Damonte M.D2, Virginia Damonte M.D2, Ana Basquiera M.D1.
1Hematology, Hospital Privado Universitario de Cordoba, Cordoba, Argentina; 2Hemotherapy, Hospital Privado Universitario de Cordoba, Cordoba, Argentina; 3Cellular Therapy, Hospital Privado Universitario de Cordoba, Cordoba, Argentina
Introduction: Autologous Stem Cell Transplantation (ASCT) remains a standard first-line treatment in eligible patients with Multiple Myeloma (MM). Graft storage for a maximum of 72 hours at 2-6 C and infusion after high dose melphalan has been increasingly used and was adopted as an option for cryopreservation in our center in 2019.
Objectives: To compare time to neutrophil engraftment (>500/ul), time to platelets engraftment (>20000/ul), days of hospital stay, engraftment failure, one-year overall survival (OS), one-year relapse-free survival (RFS), one-year relapse rate, 100-days transplant-related mortality (TRM), MM response at 100 days after transplantation, number of red blood cell transfusions, and number of platelets transfusions, between patients that received an ASCT with cryopreserved graft and those who received a graft stored at 2-6 C° (non-cryopreserved graft).
Materials and Methods: We conducted a retrospective comparative analysis of MM patients’ clinical records that received an ASCT in our center from January 2019 to April 2021. Cryopreserved grafts were stored in freezer at -80 C, DMSO and albumin were added as institutional protocol. Non-cryopreserved grafts were stored at 2-6 C° for a maximum of 72 hours after collection. The conditioning regimen was melphalan 200/140 mg/m2 administered on day -2 with cryopreserved grafts and on day -1 with non-cryopreserved grafts. Kaplan-Meier curves were used for OS and RFS analysis and the long-Rank test was used for comparisons. The cumulative incidence function was used for TRM and relapse rate analysis.
Results: From January 2019 to April 2021, 88 patients (median age 56,9 years) with MM received an ASCT in our center. 47 (53.4%) received a cryopreserved graft and 41 (46.6%) received a non-cryopreserved graft. No statistically significant difference was found between groups regarding age, sex, MM status before ASCT, number of treatments before ASCT, ISS stage, time to transplant, CD34+ dose, plerixafor use, and renal function. Conditioning regimen was melphalan 200 mg/m2 in 79 (89%) and 140 mg/m2 in 9 (11%) patients. The median time from collection to graft infusion in non-cryopreserved grafts was 45.5 hours. No statistically significant difference was found between groups with regard to time to neutrophil and platelets engraftment, number of red blood cell and platelets transfusions, OS, RFS, relapse rate, TRM, and MM response after transplant. There were no graft failure events. Patients receiving a non-cryopreserved graft had a shorter hospital stay (14 vs 15 days; p=0.008).
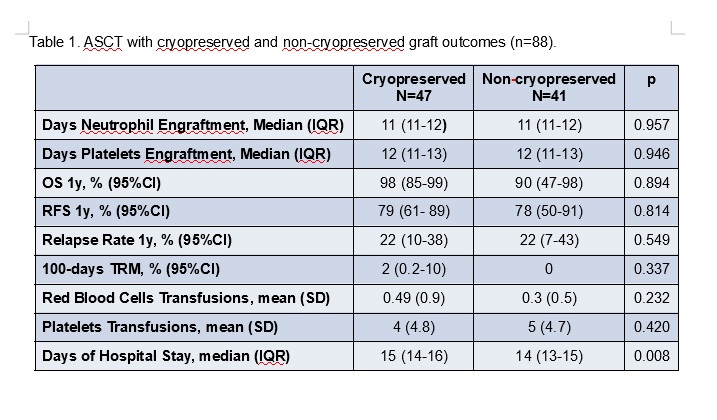
Conclusion: ASCT with non-cryopreserved graft in MM patients showed similar results to the cryopreserved modality, with a shorter hospital stay and avoiding DMSO potential toxicity.

