

Pancreas graft rejection: incidence, treatment and outcomes
Pablo Uva1,2,3, Alejandra Quevedo1, Josefina Roses1, Roxana Pilotti1, Maria F Toniolo1, Esteban C Alvarenga2, Eduardo Chuluyan3.
1Pancreas Transplantation, Instituto de Trasplantes y Alta Conplejidad (ITAC-Nephrology), Buenos Aires, Argentina; 2Pancreas Transplantation, Hospital General de Agudos "Dr. Cosme Argerich", Buenos Aires, Argentina; 3CEFyBO, CONICET, Buenos Aires, Argentina
Introduction: Pancreas rejection continues to be a major cause of graft failure (GF). Treatment protocols differ among transplant centers.
Materials and Methods: Since December 2011 pancreas biopsies are performed systematically at any graft dysfunction and pancreas rejection is treated according to rejection type and grade. The objective is to report incidence, type, grade, treatment and outcomes of pancreas rejection until March, 2022. Standard anti-rejection treatment: Indeterminate and Banff 1: Steroid pulses, Banff 2: SP+ Thymoblobulin. AMR: Steroid pulses, plasmapheresis and IVIG, Mixed rejection: SP+Thymo+PP+IVIG. However, due to kidney discordant grade or rejection and/or patient condition, treatment may have varied.
Results: We have performed 419 pancreas transplants at our center, of which 242 were performed during the study period. The incidence of rejection was 17% at 1y and 25% at 5y. We analyzed 93 pancreas biopsy proven rejections. Among the 71 first episodes, there were 4 indeterminate rejections (0% GF), 43 Banff 1 rejections (7% GF), 15 Banff 2 rejections (33% GF) 8 AMR (25% GF) and 1 chronic rejection (100% GF).
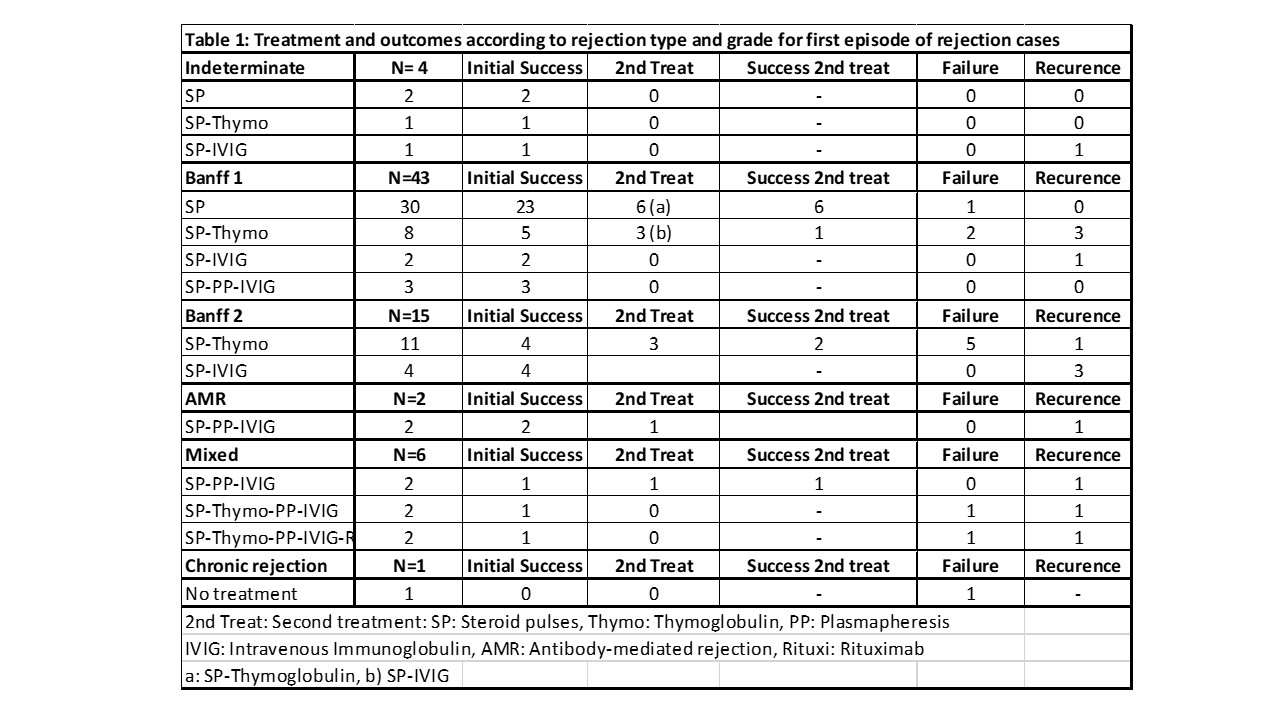
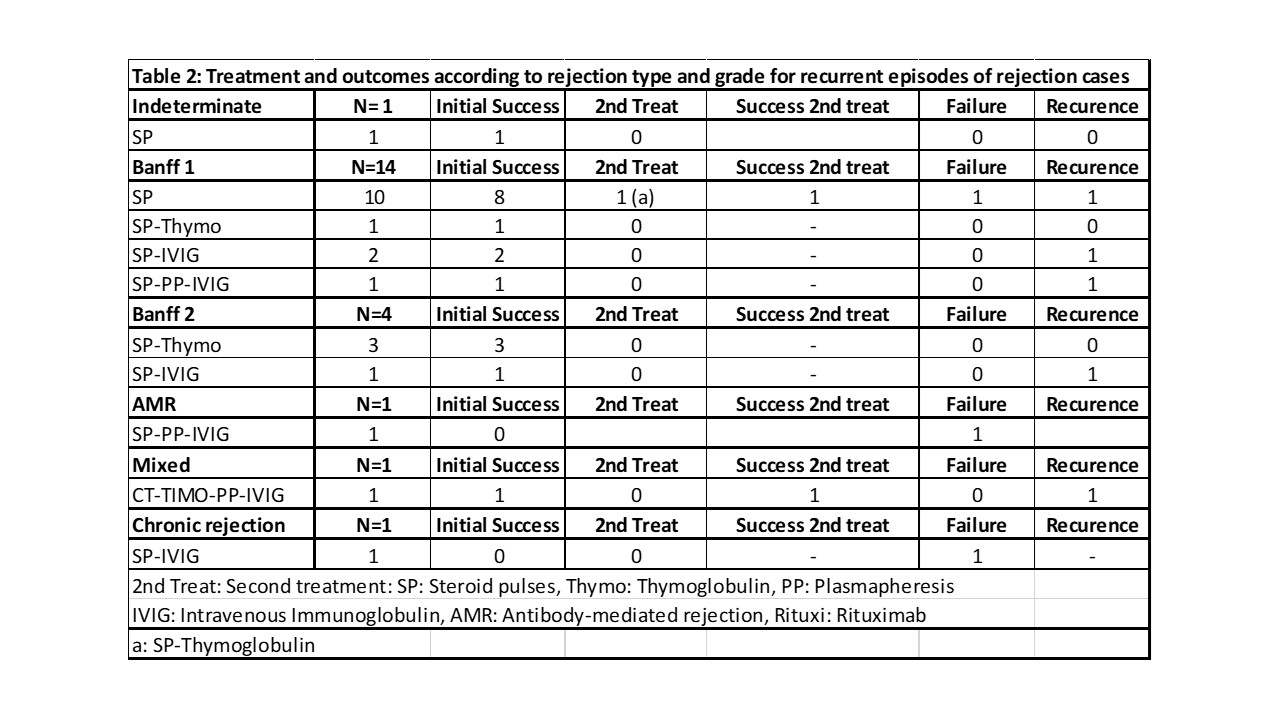
Recurence of refection after a first episode was 11% for Banff 1 and 50% for Banff 2 and AMR cases. Among the 22 episodes of recurrent rejection there were 1 indeterminate rejection (0% GF), 14 Banff 1 rejection (7% GF), 4 Banff 2 (0 % GF), 2 AMR (100% GF) and 1 chronic rejection (100% GF).
In 29 cases, a repeat biopsy was performed during the first 2 months after initial treatment confirming persistent rejection (12), resolution of rejection (16 cases) or graft failure (1 case).
Discussion: Pancreas rejection is still a prevalent complication after transplantation. Tailoring anti-rejection treatment according to pancreas pathology, kidney pathology and patient status may result in a more efficient use of immunosuppression. Repeat biopsy can assist differentiate cases or persistent rejection vs resolution of rejection when elevated enzymes or hyperglycemia persists after treatment.

