
Long-term rejection free renal allograft survival with Fc-modified anti-CD154 antibody monotherapy in nonhuman primates
Grace Lassiter1, Takayuki Hirose1, Ashley D'Attilio1, Ahmad Karadagi1, Ryo Otsuka1, Toshihide Tomosugi1, Tatsuo Kawai1.
1Center for Transplantation Sciences, Massachusetts General Hospital , Boston, MA, United States
Belatacept is currently an only FDA approved costimulatory blockade (CB) used as an alternative to calcineurin inhibitors in kidney transplantation. However, it has been associated with higher rates of acute cellular rejection (ACR) and more effective CB has been sought. Blockade of the CD154/CD40 pathway with anti-CD154 antibody (aCD154) has been shown to be more effective in inhibiting alloimmune responses than CTLA4Ig. Unfortunately, clinical application of aCD154 has been abandoned due to its thrombophilic property which appears to be mediated by FcγRIIA receptor–dependent platelet activation. To address this problem, an Fc-modified aCD154 (TNX-1500), in which Fc was engineered to decrease binding to Fcγ RII, has been developed. In the current study, we have evaluated TNX-1500 for its efficacy to prevent kidney allograft rejection in NHPs.
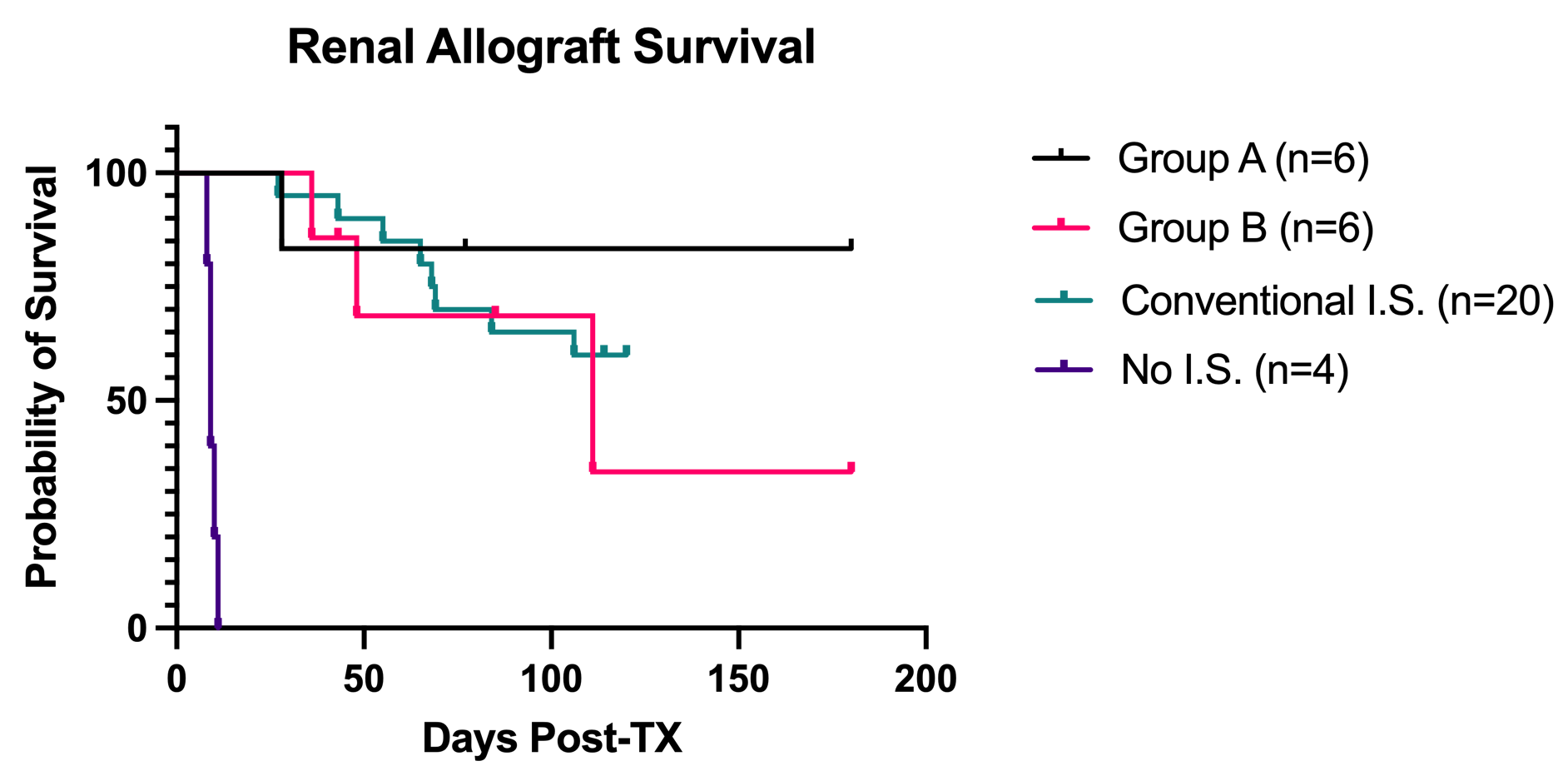
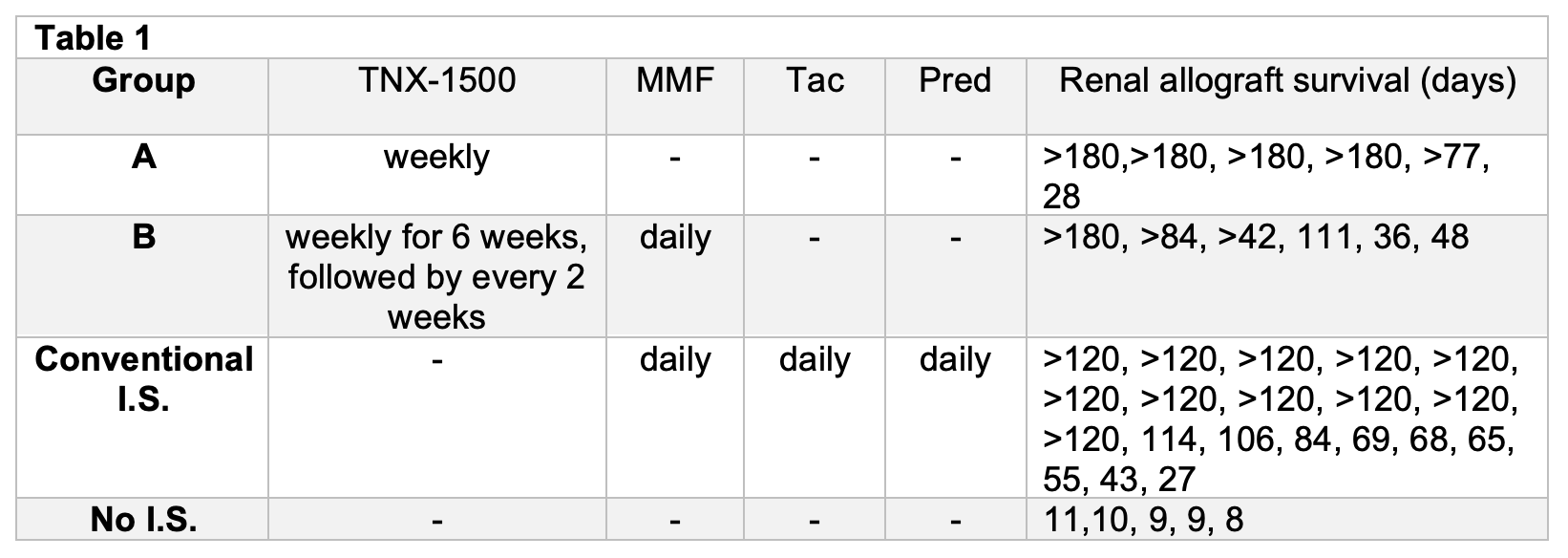
Twelve cynomolgus macaques received MHC mismatched kidney allografts with either TNX-1500 monotherapy (20mg/kg weekly) (Group A) or combined with daily mycophenolate mofetil (MMF) (TNX-1500 weekly for 6 weeks followed by every 2 weeks) (Group B). The results were compared with our historic results of no immunosuppression (No IS, n=5) or conventional immunosuppression (I.S.) with tacrolimus (Tac), MMF and methylprednisolone (Pred). (Conventional IS, n=20).
Without any prophylaxis, no thromboembolic complication was observed in all nine recipients of TNX-1500. Renal allograft survival at 6 month was 80% in Group A (n=6). Histopathology at 6 months of 5/6 recipients showed no evidence of rejection (g0,i0,t0,v0,ptc0,cg0,ci0,ct0,cv0, C4d0). One recipient lost on day 28 with ACR2b. Six recipients have so far have been tested in Group B. Two recipients developed rejection on day 36 and 48 while they were still treated with weekly TNX-1500. Another recipient had to be euthanized on day 111 post-transplant due to complications from MMF. The three other recipients in this group are currently in progress with normal kidney function at days >180, >84 and >42. Renal allograft survival at four months in Conventional I.S. was 52% (p=0.33 vs. Group A) and all five recipients without I.S. rejected their kidney allografts by day 11 (p=0.0018 vs. Group A).
Excellent renal allograft survival was achieved with TNX-1500 monotherapy without thromboembolic complications. Combination with MMF resulted in inferior allograft survival.
Financial support from NIH Grants 1R21AI163806-01, 5T32AI007529-22 & Tonix Pharmaceuticals.

