

Donor-derived cell free DNA is associated with antibody-mediated rejection and impaired cardiac hemodynamics in patients with heart transplantation
Giosafat Spitaleri1, Laura Borgese1, Laura Giovannini1, Arianna Orsini2, Bianca De Nicolo2, Maria Francesca Scuppa1, Antonio Russo1, Marco Masetti1, Paola Prestinenzi1, Mario Sabatino1, Elena Bonora2, Ornella Leone3, Luciano Potena1.
1Heart Failure and Transplant Unit, IRCCS Azienda Ospedaliero-Universitaria di Bologna, Bologna, Italy; 2Unit of Medical Genetics Department of Medical and Surgical Sciences, University of Bologna, Bologna, Italy; 3Unit of Pathology, IRCCS Azienda Ospedaliero-Universitaria di Bologna, Bologna, Italy
Introduction: Donor-derived cell-free DNA (ddcfDNA) has emerged as a non-invasive biomarker for the detection of acute cellular rejection (ACR) and antibody-mediated rejection (AMR) in heart transplant (HT) recipients. Nevertheless, data regarding the clinical application of this method in a real-life setting are lacking. The aim of the present study is to assess the relationship between ddcfDNA levels, ACR, AMR and cardiac hemodynamic parameters in a European real-life cohort of HT recipients.
Method: Among the patients who received a protocol or for-cause endomyocardial biopsy (EMBx) in the period 2017-2021 at our center, we selected those with available biobanked plasma as part of the CLIN-HEART registry. ddcfDNA was measured using MiSeq Illumina platform, according to the AlloSeq cfDNA protocol (CAREDx, San Francisco, CA, USA). Pulmonary arterial wedge pressure (PAWP), right atrial pressure (RAP) and cardiac index (CI) were assessed at the time of the EMBx. Significant rejection was defined as ACR grade ≥2 and AMR grade ≥1, according to International Society for Heart and Lung Transplantation classification.
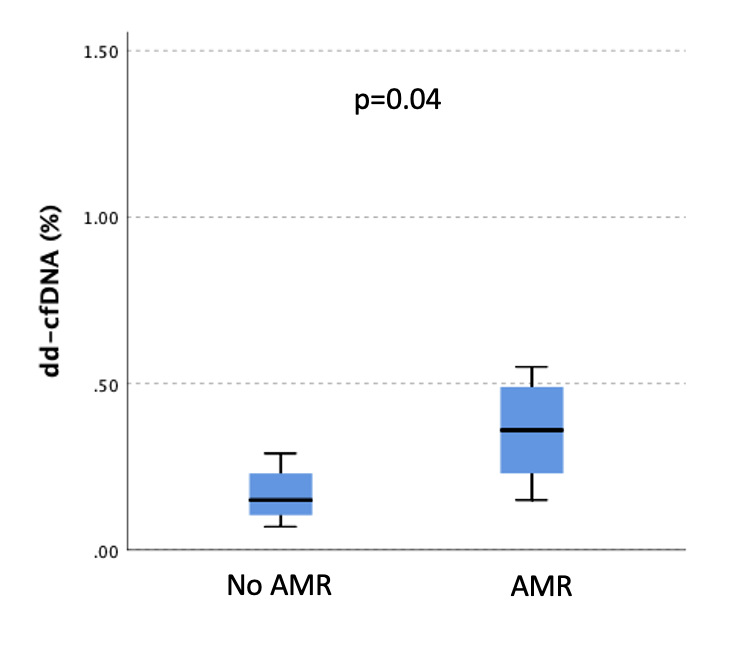
Results: DdcfDNA assessment was performed in 66 recipients. Median ddcfDNA levels were significantly higher during the first month after HT (0.33% [IQR 0.19 to 0.47] in the first 30 days vs. 0.17% [IQR 0.12 to 0.23] after 30 days from HT, p=0.004). Rejection was detected in 19 (28.8%) patients, in whom median ddcfDNA levels were 0.23% (IQR 0.16 to 0.38%). Starting from 30 days after HT, ddcfDNA levels were higher in recipients with AMR (p=0.04, Figure 1) as compared to those without.
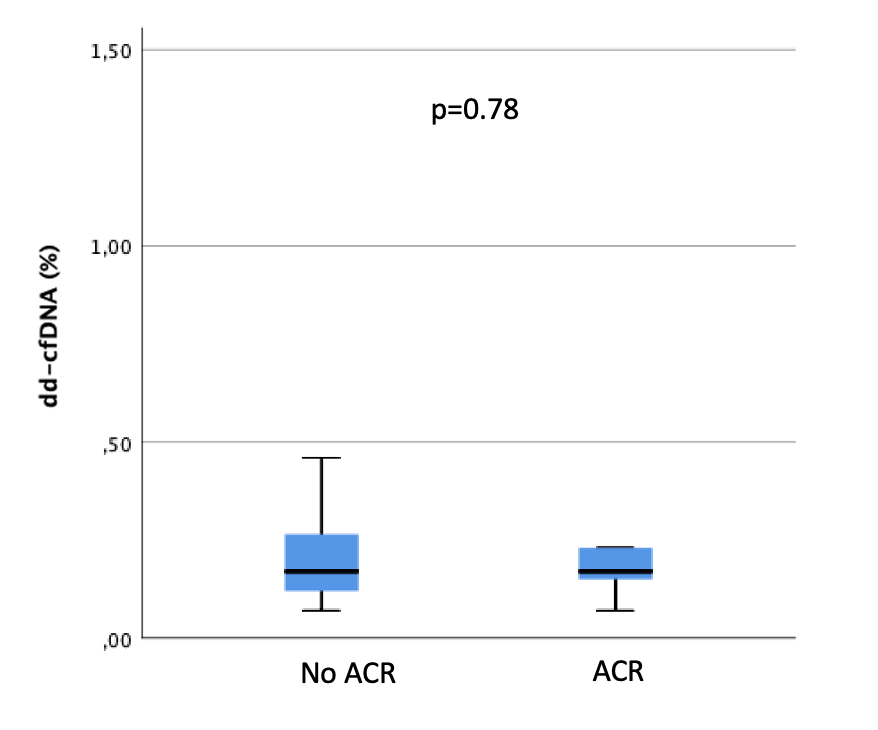
However, no significant relationship was found between ACR and ddcfDNA levels (p=0.78, Figure 2). With regards to cardiac hemodynamics, HT recipients with rejection and ddcfDNA levels above the median had a higher PAWP (15 mmHg [IQR 14 to 17 mmHg] vs. 10 mmHg [IQR 8 to 13 mmHg], p=0.04) and RAP (9 mmHg [IQR 7 to 11 mmHg] vs. 4 mmHg [IQR 2 to 6 mmHg], p=0.03), but not CI (3.07 l/min/m2 [IQR 2.90 to 3.58 l/min/m2] vs. 3.28 l/min/m2 [IQR 2.62 to 4.29 l/min/m2], p=1.00), as compared with those with ddcfDNA levels below the median. Conversely, in recipients without rejection, there was no significant association between ddcfDNA and PAWP, RAP nor CI.
Conclusions: In a European real-life cohort of HT recipients, ddcfDNA levels were higher during the first month after HT and decreased thereafter. Starting from 30 days after HT, AMR but not ACR was associated with higher ddcfDNA levels. Finally, high ddcfDNA levels were associated with hemodynamic derangements only in patients with rejection.

