
Torque Teno virus titre changes under immunosuppression reduction protocol for BK virus-associated nephropathy: a single centre pilot study
Ramyangshu Chakraborty1, Jon Bible2, Michelle E Allan1, Tasnuva Kashem1, Gregor Young1, Maha Mohamed1, David Randall1, Raj Thuraisingham1, Stanley Fan1, Ismail Mohamed1, Kieran McCafferty1, Teresa Cutino-Moguel2, Muhammad Magdi Yaqoob 1.
1Department of Renal Medicine and Transplantation, Royal London Hospital, Barts Health NHS Trust, London, United Kingdom; 2Department of Virology, Barts Health NHS Trust, London, United Kingdom
Introduction: In BK virus-associated nephropathy (BKVaN), balancing the risk of immunosuppression (IS) reduction with the potential benefits can be challenging. A common approach is to empirically stop antiproliferative agents in the first instance and reduce the dose of calcineurin inhibitors (CNIs) later. Torque Teno virus (TTV), a novel ubiquitous DNA virus, has emerged as a better predictor of IS burden in some studies. We examined the changes in BKV and TTV titres in response to IS reduction as part of BKVaN treatment.
Method: 20 renal transplant patients with stored blood samples were included in the study cohort from a population transplanted between 2017-19, in remission from an episode of clinically significant BK viraemia. They received standard IS; tacrolimus, antiproliferative (mycophenolate mofetil/azathioprine) and weaning dose prednisolone. BKV and TTV titres, 30-day average tacrolimus concentration, the dose of antiproliferative and prednisolone were collected at 4-time points. These included the last negative BK PCR; the onset of viraemia; the peak BK titre and BK titre <500 copies/ml. TTV DNA was extracted from stored frozen plasma and PCR was performed with Thermofisher 7500 Fast platform and TTV R-GENE® kit. The relationships between the variables were assessed using a multivariable linear regression model. Data were collected from electronic patient records and analysed with R 4.0.3.
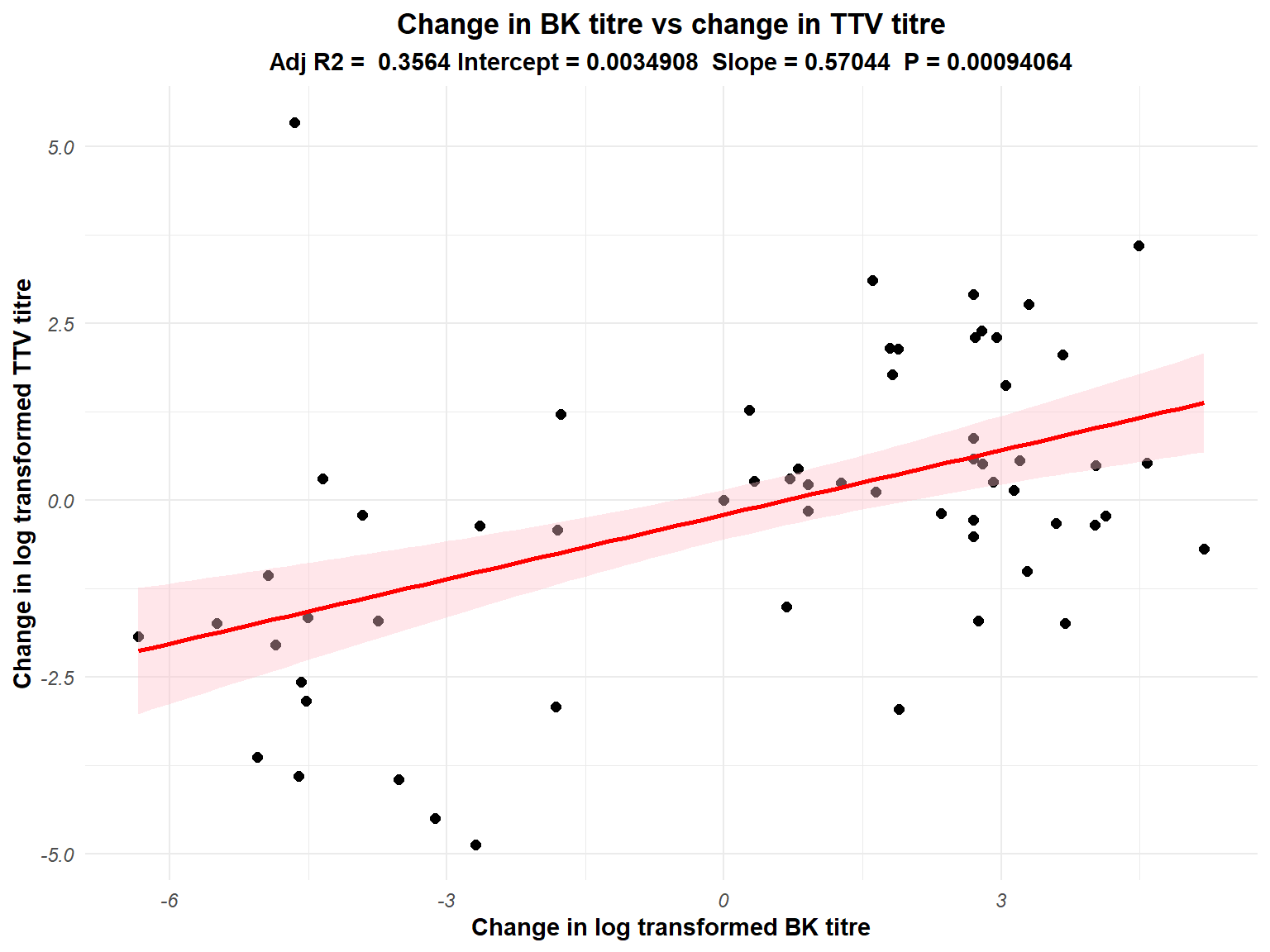
Result: The log-transformed mean TTV titre at the 4 time points were 5.02 (2.07), 5.52 (1.74), 6.23 (2.14) and 4.56 (1.27) respectively. In the multivariable model, log-transformed BK virus titre increased by 0.25 for every 1 ng/mL increase in tacrolimus concentration (p 0.0008). However, every 1 log rise in TTV titre led to 0.57 (0.17) log copies increase in BKV titre (p 0.0009), once adjusted for tacrolimus concentration. The relationship between tacrolimus and BKV became statistically insignificant when TTV titre was added as a predictor variable. This implies that TTV titre is a more sensitive predictor of BK viral load than tacrolimus concentration. Although statistically significant, all changes in antiproliferative or prednisolone dose were unable to predict linear changes in BKV titres. 5 patients who lost their graft in the mean follow up of 2.8 years had significantly low TTV titres (p< 0.05) at baseline, indicating suboptimum IS burden. In this small cohort, there was no relationship between TTV titres and rejections (n=5) or de novo DSA (n=3). An ongoing adequately powered prospective study will address these questions more decisively.
Conclusion: Our study demonstrates that TTV titres more accurately indicate the effect of IS/CNI changes on BK titre and demonstrates its potential as a sensitive assay to objectively guide IS modification compared to current empirical practice in the management of BKVaN. A randomised control trial is warranted comparing empirical practices to TTV titre guided adjustment of immunosuppressive medications.

right-click to download