
Four-year patient survival after simultaneous pancreas-kidney transplantation according to graft status using Kaplan-Meier survival method versus competing risk model
Lucia Alfaro Villanueva 1, Jose Medina-Pestana1, Laila Viana 1, Marina Cristelli 1, Erika B Rangel1, Helio Tedesco-Silva 1, Roberto F Meirelles 1.
1Renal Transplantation Program, Hospital do rim - Fundação Oswaldo Ramos, Sao Paulo , Brazil
Background: Cardiovascular events and infections are the leading causes of death after simultaneous pancreas-kidney transplantation (SPKT). Previous studies have shown the graft loss is also related to overall patient survival probability; however, the survival analyses by traditional methods can face bias due to not considering the competing risk between graft losses and death.
Aim: To compare the patient survival submitted to SPKT according to the status of graft losses, kidney, pancreas, or both four years after transplantation.
Methods: This is a retrospective, longitudinal and observational study that enrolled 432 patients submitted to SPKT at Hospital do Rim between 2000 and 2015. The final date follow-up was December 2019. The patients were categorized into four groups according to the graft status: renal graft loss (RL), pancreas graft loss (PL), both grafts losses (BL), and no graft loss (NL). 1- and 4-year patient survivals were analyzed by Kaplan-Meier and competing risk model. The association between graft loss and patients' survival was estimated by univariable and multivariable models thorough Cox regression, considering NL as a reference group.
Results: The frequency of patients and time to graft loss according to groups were: 3.7% for RL, in 14.7 months; 10.6% for PL, in 0.67 months; and 8.6% for BL, in 1.5 and 1.37 months for the pancreas and renal graft losses, respectively. After four years of follow-up, 77.1% of patients had both functioning grafts. The 1- and 4-year patients' survival by Kaplan-Meier were 85.8% and 80.7%, respectively, with no differences between PL and NL, 86.5% e 93.4%; however, they were significantly higher than BL and RL, 25.4% and 43.7%, respectively (P<0.001). The age-adjusted risk of death was associated with RL (HR=5.70; P<0.001) and BL (HR=9.60; P<0.001). The results of 1- and 4-year patient survivals by competing risk model were near to those observed by the Kaplan-Meier method for RL, PL, and NL; however, for BL, the survival probability was higher when analyzed by competing risk: 40.5% vs. 52.4%, and 25.4% vs. 32.6%, one and four years, respectively. Similarly, in the Cox regression by competing risks, RL (HR= 5,09; P<0,001) and BL (HR=9.65; P<0,001) significantly increased the likelihood of patients' death in four years of follow-up.
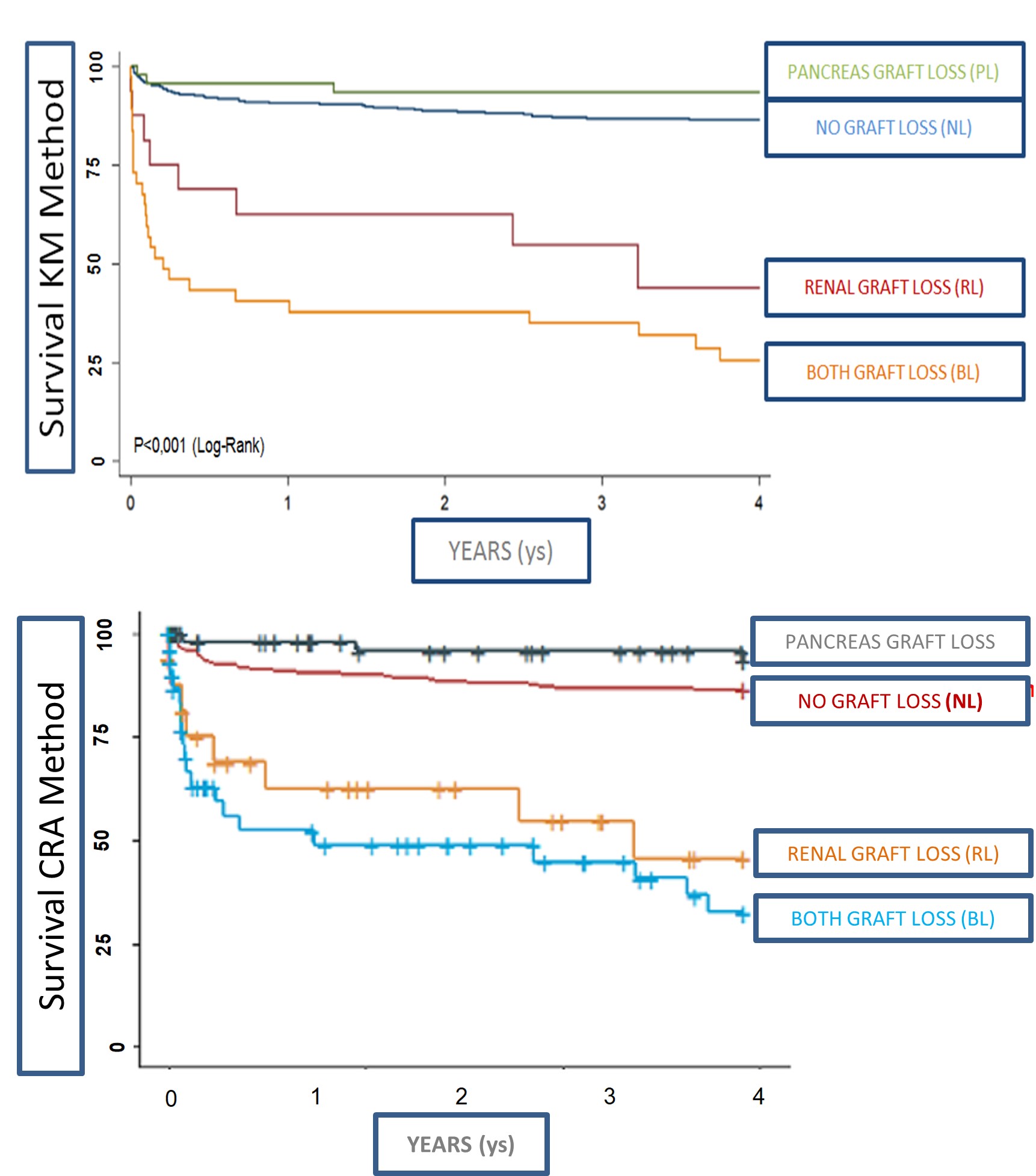
Conclusion: The renal graft loss or the losses of both graft, kidney, and pancreas significantly impacted the survival probability of patients submitted to SPKT four years after transplantation, and this pattern was observed as by Kaplan-Meier method, as by competing risk model.

right-click to download