
Portal-endocrine and gastric-exocrine drainage technique in pancreas transplantation
Hosein Shokouh-Amiri1, Muhammad S Naseer1, Robert McMillan1, Donnie Aultman1, Srijan Tandukar1, Neeraj Singh1, Gazi B Zibari1.
1Transplant, John C. McDonald Regional Transplant Center - Willis Knighton Health System, Shreveport, LA, United States
Background: Diagnosis of rejection has continued to be problematic in pancreas transplantation (PT). In 2007, we innovated a new surgical technique for PT, portal-endocrine and gastric exocrine drainage (P-G) technique, where the end of allograft jejunum was anastomosed to the anterior aspect of the stomach, facilitating endoscopic access to duodenum/pancreas allograft.
Objective: The aim of our study was to evaluate the safety, measure allograft rejection, and calculate graft and patient survival in patients who underwent PT with the P-G technique.
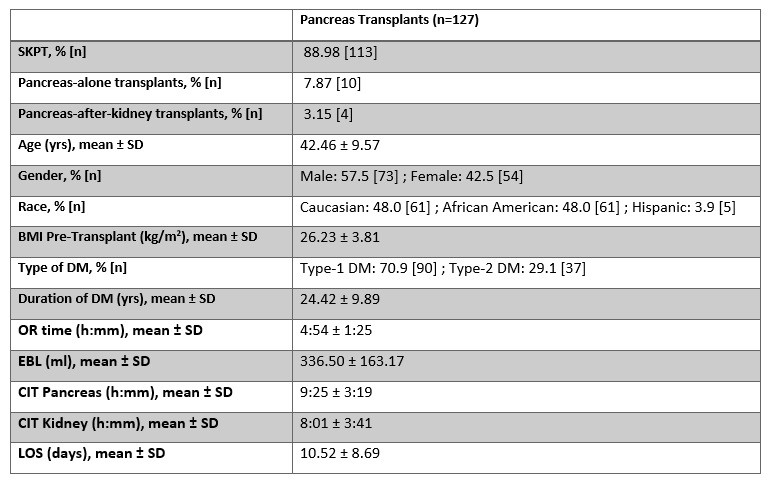
Method: This was a retrospective review study of 127 PT patients with the P-G technique from Sep 2007 to Dec 2021 at our center. 113 simultaneous kidney-pancreas transplants (SKPT), 10 pancreas-alone transplants, and 4 pancreas-after-kidney transplants were performed. Baseline demographics, OR time, estimated blood loss (EBL), cold ischemic time (CIT) for kidney and pancreas allografts, length of hospital stay (LOS), complications, number of patients with endoscopy, number of patients with allograft rejection, death-censored 5-year kidney and pancreas graft survival, and 5-year patient survival were calculated.
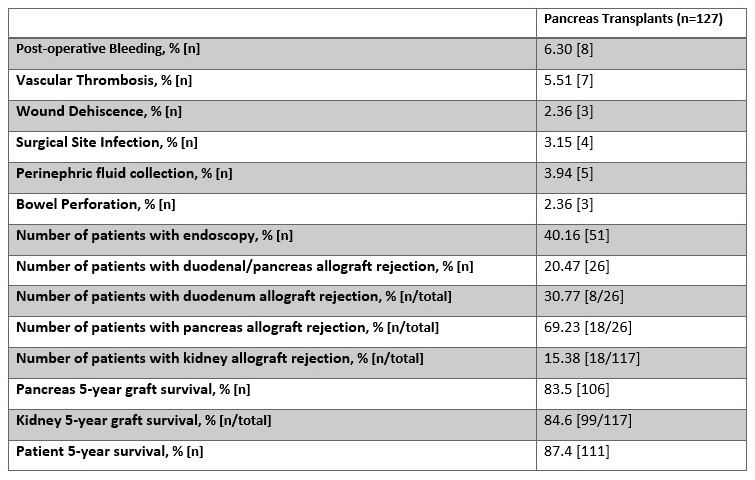
Results: Table 1 summarizes baseline demographics and Table 2 highlights complications and outcomes. Perioperative complications included 8 post-operative bleeds and 7 vascular thromboses. Patients with vascular thrombosis had subsequent transplant pancreatectomies within 6 weeks. During the study period, 51 transplant patients underwent upper GI endoscopy. Duodenum/pancreas allograft rejection was found in 26 patients. The death-censored 5-year graft survival for pancreas and kidney were 83.5 % and 84.6 %, respectively. Patient survival was 87.4%. Figure 1 shows the Kaplan-Meier curves for pancreas graft, kidney graft, and patient survival.

Conclusion: This P-G drainage technique for PT has proven to be safe with comparable graft and patient outcomes. Access to donor duodenum and pancreas allograft via endoscopy is unique to this technique and provides the added advantage of life-long easy access to the allograft.

right-click to download