

Graduated in Medicine at the Faculty of Medical Sciences of Santos (1980), Masters in Pediatrics at the Federal University of São Paulo (1991), Ph.D. in Pediatrics at the Federal University of São Paulo (1994), and post-doctoral training in Pediatrics at the Claude Bernard de Lyon, France (1996-1997). For 25 years worked as a professor at the Faculty of Medical Sciences of Santos, where was head of the Department of Maternal and Child Health. Since 2007 working as a professor at the Department of Pediatrics at the Federal University of São Paulo-Escola Paulista de Medicina, working in the Pediatric Nephrology sector. Since 2008 working as coordinator of the Kidney Transplant Service at the Hospital Samaritano Higienópolis in São Paulo. Experience in Medicine, with an emphasis in Pediatrics, working mainly on the following topics: pediatric nephrology, kidney transplantation, and pediatric intensive care.
Long-term results of kidney transplantation in children with bodyweight lower than 10 Kg
Paulo C. Koch Nogueira1,2, Luciana Feltran1,2, Maria Fernanda Camargo1.
1Pediatric Transplantation, Hospital Samaritano de Sao Paulo, São Paulo, Brazil; 2Pediatrics, UNIFESP, São Paulo, Brazil
Objective: To evaluate long-term results of kidney transplantation comparing low weight (<=10 Kg) to bigger children.
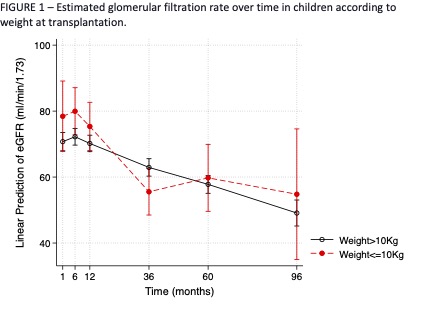
Methods: Unicentric cohort involving children who underwent kidney transplantation. The primary clinical outcomes were the 7 years death-censored graft survival, and the estimated glomerular filtration rate (eGFR) at 1, 3, 5, and 7 years. The main risk variable was weight at transplantation and children were categorized as G1: <= 10Kg and G2 > 10Kg. Covariables were CKD etiology, and kidney donor type (living/deceased). The survival estimates were fit through univariate and multivariable Cox regression models, and the eGFR over time was modeled using multilevel mixed-effects linear regression.
Results: The study involved 451 first kidney transplants in children (53 from G1 and G2 398 from G2), with a median age of 7.6 (4.0 to 12.5) years, 64% male, 53% CAKUT. G1 had a) more living related donors (28% versus 17%), and b) slightly different CKD etiologies, with more CAKUT (64% versus 52%) and hereditary diseases (23% versus 13%), both results tending towards a significant difference (p=0.06 in both cases). Graft survival at 7 years was 86% (75 to 99) in G1 and 84% (79 to 88) in G2 (p=0.791). The mixed-effects model revealed that both groups had a significant decline in eGFR over time (p<0.001), but with no significant difference (p=0.172) between groups (FIGURE 1). To adjust for the higher proportion of living donors in G1, we analyzed separately the subgroups according to kidney donor type, and these analyses did not change the results of the models.
Conclusions: The main finding of this study is the similar long-term results of kidney transplantation in both groups. This results in a sizeable number of low-weight children should uphold kidney transplantation in small children.

right-click to download