
Which oxygen concentration is best for renal normothermic machine perfusion: hyperoxia or normoxia?
Veerle Lantinga1, Tim L. Hamelink1, Baran Ogurlu1, Isa M. Tricht1, Jasper G. Leengoed1, Henri G.D. Leuvenink1, Cyril Moers1.
1Surgery, University Medical Center Groningen, Groningen, Netherlands
Introduction: Normothermic machine perfusion (NMP) of renal grafts provides a platform for organ evaluation and regeneration. However, there is no consensus about the oxygen concentration that should be applied. Typically, a 95%O2/5%CO2 gas mixture is used, resulting in a supra-physiological partial oxygen pressure of 60-80 kPa. Such hyperoxia can potentially promote the formation of reactive oxygen species (ROS) and thus worsen ischemia-reperfusion injury of the graft. We hypothesized that NMP with normoxia (pO2 10-20 kPa) may prevent additional ROS-induced renal injury, which could be associated with more favourable perfusion parameters and a better metabolic rate.
Materials and Methods: Paired renal grafts from 8 pigs were procured at the local slaughterhouse and stored on oxygenated hypothermic machine perfusion for 10 hours. The left and right kidney were randomized to either 6 hours of NMP with hyperoxia (70kPa, n=8) or 6 hours of NMP with normoxia (10-20 kPa, n=8). Biopsies were taken at the end of HMP and after 1 hour, 3 hours and 6 hours of NMP. Perfusate and urine samples were taken hourly, and perfusion parameters were monitored continuously.
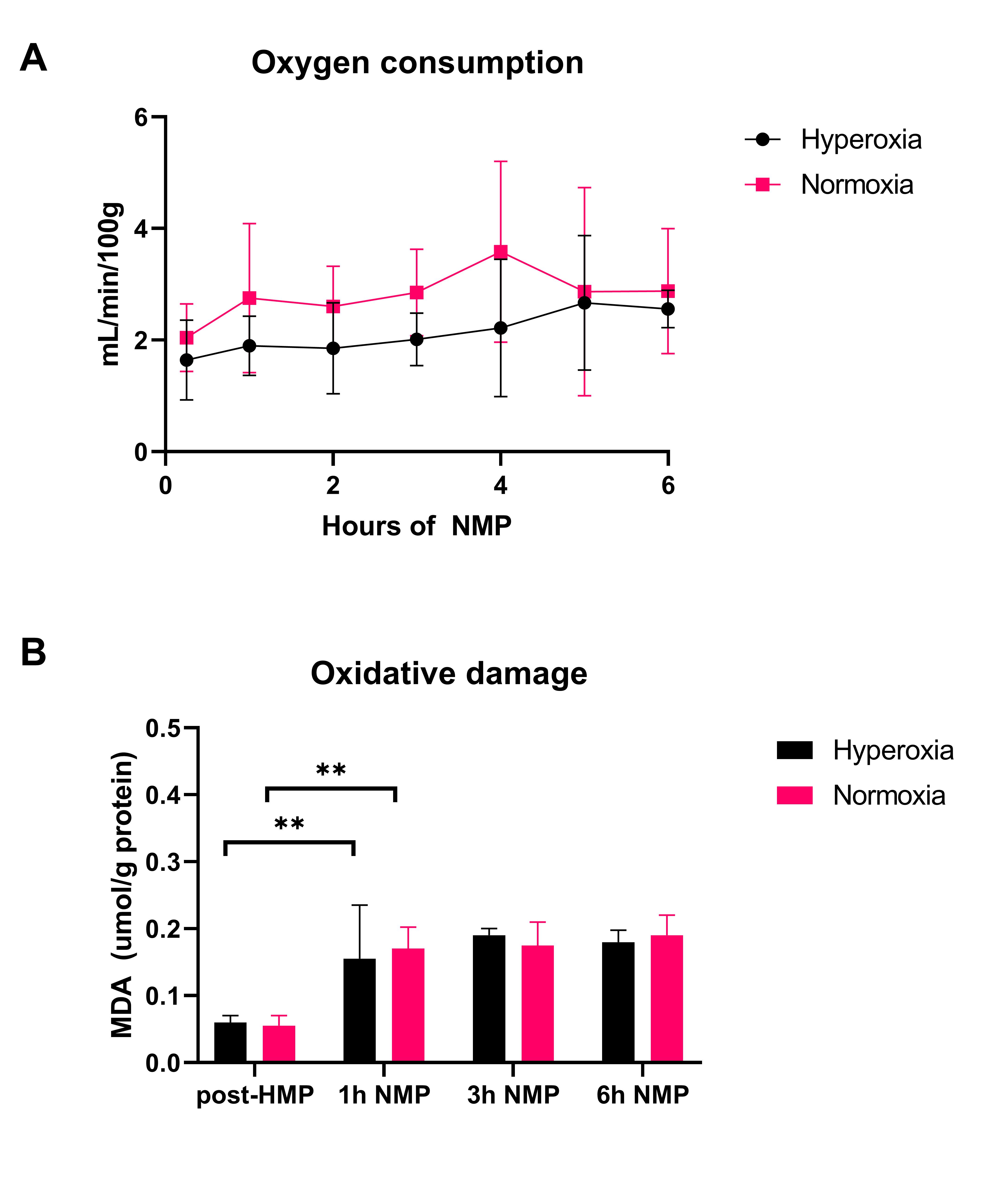
Results: Kidney function, measured as creatinine clearance and fractional sodium excretion was similar for both groups. Likewise, perfusate injury markers were similar for both groups. Total oxygen consumption tended to be higher in the normoxia group (p=0.08) (Figure 1A), and tissue ATP levels were similar at all timepoints. Oxidative stress measured by malondialdehyde (MDA) formation increased significantly after initiation of NMP (p<0.01), but did not differ between both groups at all timepoints (Figure 1B).
Conclusion: No significant differences in kidney function, damage markers and oxidative stress were seen between the kidneys exposed to hyperoxia and normoxia during renal NMP. Therefore, we conclude that hyperoxia during renal NMP does not lead to increased ROS-induced injury compared to normoxia.

right-click to download