
Outcomes and risk of recidivism after deceased and living donor liver transplant for alcoholic liver diseases
Tiffany Wong 1, Chung Mau Lo1.
1Surgery , The University of Hong Kong, Hong Kong, People's Republic of China
Background: Alcoholic liver disease (ALD) is one of the commonest indication for liver transplant (LT). Limited data in literature on the outcomes of these patients after living donor (LDLT) and deceased donor liver transplant (DDLT). This study aimed to evaluate the survival outcomes on waitlist, after LT and risk of recidivism.
Method: This was a retrospective study from a university center. All data was retrieved from a prospectively collected database. All liver transplant canddiates who had ALD and underwent transplant evalution from 2008 to 2021 were analyzed. Patients were divided into 2 groups. For candidates who had at least one eligible live donor, they would be considered as "intention-to-treat LDLT" (ITT-LDLT), whereas patients who did not have live donor would be considered as "intention-to-treat DDLT". Patients who were not accepted for either LDLT and DDLT belonged to control group. Patients who were listed for DDLT must fulfill a 6-month abstience rule whereas patients who opted for LDLT could proceed to LT if they had a favorable psychological assessment and good social support. The primary outcome was survival fromt the time of evaluation. Secondary outcomes included waitlist outcomes, operative outcomes post-transplant survival.
Results: During study period, 211 ALD patients were evaluated and 86 (40.8%) did not pass medical or psychological assessment. The waitlist outcomes were listed in Figure 1. 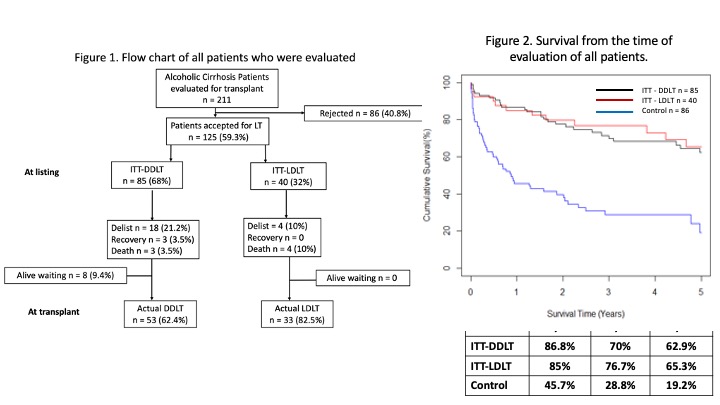
The chance of reaching LT was higher in ITT-LDLT (82.5%) when compared to ITT-DDLT (62.4%, P=0.03). Table 1 showed the baseline characteristic at time of evaluation. Control patients had the worst survival whereas there was no difference in patient survival between the ITT-LDLT and ITT-DDLT group. (Figure 2).
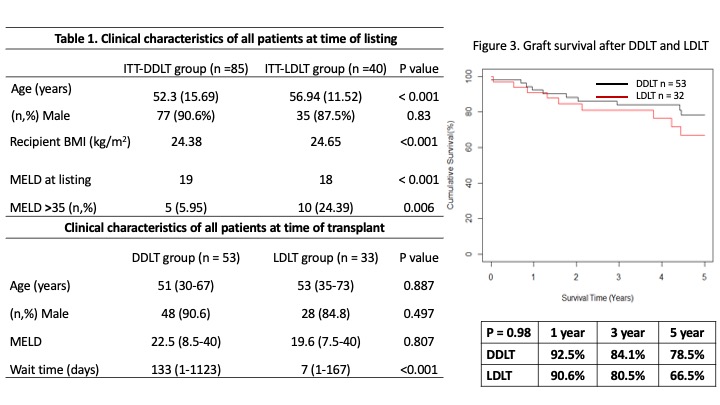
The waiting time was shorter in ITT-LDLT patients. 86 patients had LT (DDLT n=53, LDLT n=33) and patients median age, gender and MELD were similar between the 2 groups. More LDLT patients were either hospitalized (n=15, 45.5%) or required ICU support (n=6, 18.2%) when compared to DDLT patients (hospitalized n=12, 22.6% and ICU n=5, 9.4%, P=0.016). Hospital mortality (1.9% vs. 6.1%, P=0.556) and severe complication rate (45.3% vs. 36.4%, P=0.415) were similar after DDLT and LDLT respectively. Graft survival rates were similar as well. The risk of alcohol recidivism was higher after DDLT though it was not statistically significant (22.6% vs. 9.1%, P=0.107).
Conclusion: LDLT allowed a quicker access to LT and achieved similiar perioperative and long term outcomes for ALD patients.

right-click to download