
Normothermic machine perfusion (NMP) improves access to transplantation for late liver re-transplant candidates
Dimitri Sneiders1, Hanns Lembach1, Angus Hann1, Anisa Nutu1, James Hodson3, John Isaac1, Rhiannon Taylor2, Matthew Armstrong1, Thamara Perera1, Hermien Hartog1.
1The Liver Unit, Queen Elizabeth Hospital, Birmingham, United Kingdom; 2NHS Blood and Transplant, Bristol, United Kingdom; 3Institute of Translational Medicine, Queen Elizabeth Hospital, Birmingham, United Kingdom
Introduction: Late liver re-transplantation (LLrT) is a complex surgical procedure. Candidates for LLrT spend longer on the waitlist than primary transplant candidates due to selectivity in accepting organ offers. A service design using NMP was implemented in October 2018 at a single centre to facilitate increased organ utilisation of marginal organs for high-risk recipients. The aim of this study was to assess if this intervention improved access to transplantation.
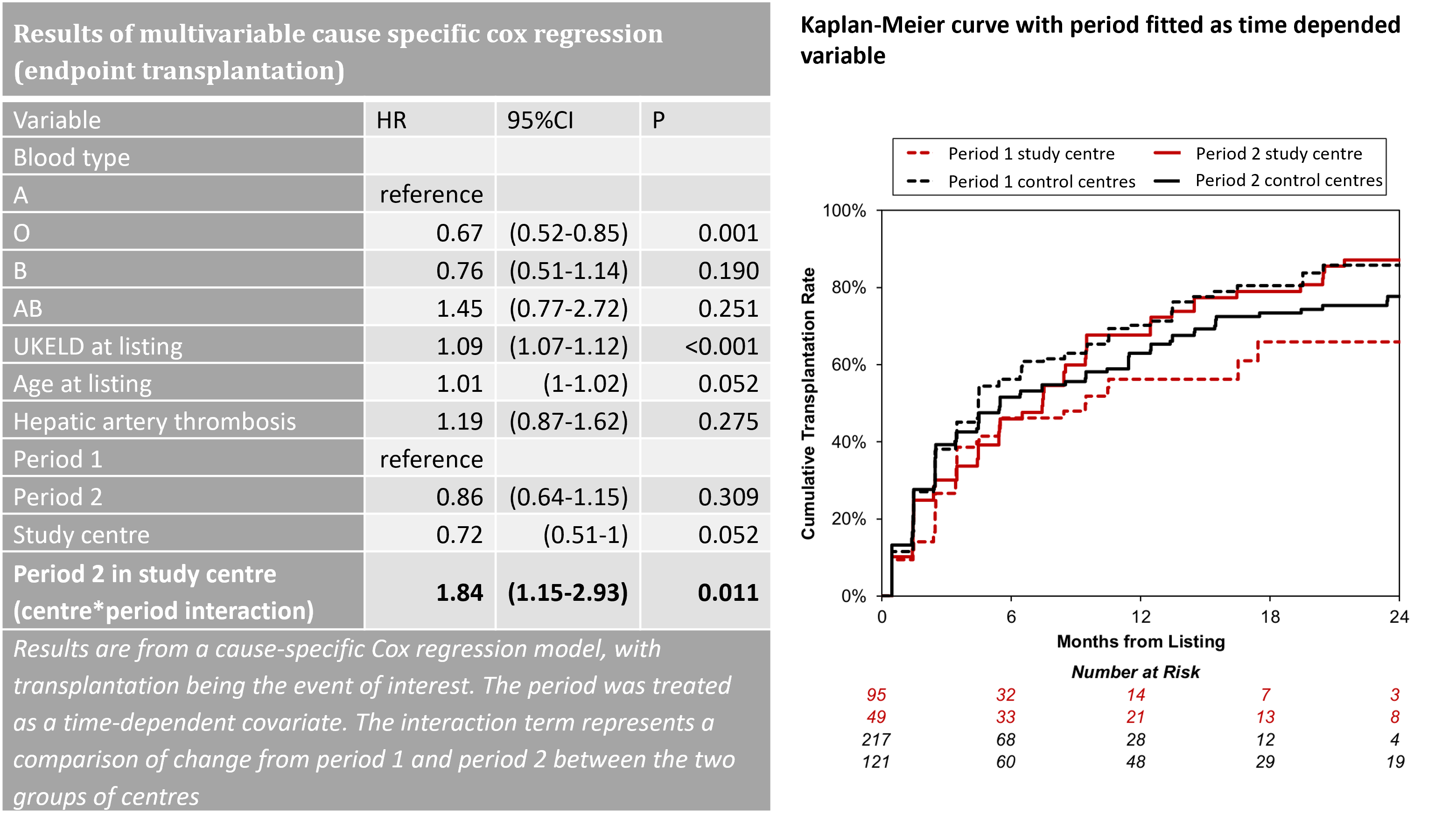
Methods: Adult patients electively listed between 2015 and 2020 for LLrT were identified from the national transplant authority database. Transplant rates prior to (period 1) and after (period 2) local implementation of the NMP service design (October 2018) were compared at the study centre and compared to the collective data from other UK centres. A cause-specific Cox regression model was used, with the period modelled as a time-dependent covariate, and the period*centre interaction being the primary factor of interest. The model was corrected for UKELD, age, indication, and blood type. Post-transplant graft survival was assessed with univariable cox regression.
Results: A total of 144 and 338 LLrT candidates were listed in the study and control centres respectively. At the study centre, the likelihood of transplantation within one year of listing increased from 56% to 68%, whilst a reduction in the LLrT rate was observed at other centres (Figure). Multivariable analysis, showed improved transplant access at the study centre in period 2 (period*centre interaction: HR: 1.83, 95%CI: 1.15-2.9, p=0.01). Post-transplant graft survival was not affected by the intervention (HR: 1.06, 95%CI: 0.41-2.69, p=0.903).
Discussion: Implementation of the NMP service design significantly improved access to transplantation for LLrT candidates, without compromising graft survival. While organ utilisation benefit for NMP has been demonstrated before, this is a first study showing a direct patient benefit of NMP for patients with long expected waiting times.

right-click to download