
Ethnic variation in human leukocyte antigen coverage by single antigen testing panels: implications for clinical applications
Justin Quon1, Jondavid Menteer1,2, Nicholas Fotiadis2, Rachel Lestz1,2, Molly Weisert2, Lee Ann Baxter-Lowe1,2.
1Keck School of Medicine, Los Angeles, CA, United States; 2Children's Hospital Los Angeles, Los Angeles, CA, United States
Introduction: Modern tests for HLA antibodies usually involve single antigen reagents, but clinically significant HLA antibodies may not be detected if their epitopes are not included in the reagents. Reagents from two vendors were examined to determine antigen coverage in eight ethnic populations: Hispanic (HIS), Native American (NAM), African American (AFA), Asian and Pacific Islander (API), Middle Eastern and North Coast of Africa (MENA), European (EUR), and mixed or unknown ethnicity (UNK).
Methods: HLA-A, -B, -C, and -DRB1 allele frequencies of each ethnic population were determined using the Common, Intermediate, and Well Documented HLA allele catalog (v3.0). For each ethnicity, the percentage of alleles not represented in single antigen reagents from two common suppliers (Vendor 1 and Vendor 2) was calculated and compared.
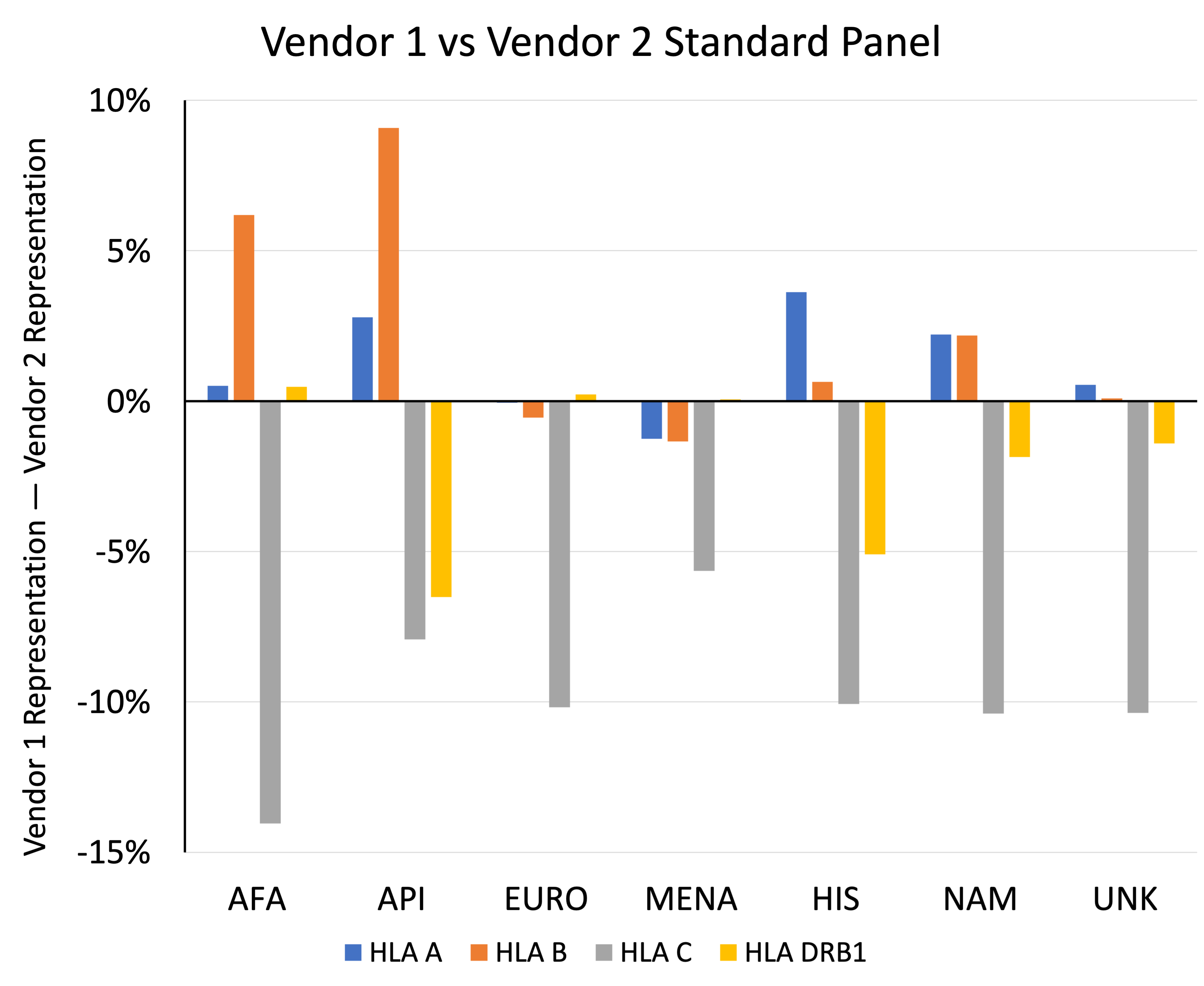
Results: Antigen coverage between single antigen reagents from the two vendors differed depending on ethnicity and HLA locus, with a maximum differential of 14.0%. For the HLA-A locus, Vendor 1 better represents the HIS, API, and NAM populations, with 3.6%, 2.8%, and 2.2% greater representation than Vendor 2, respectively. At the HLA-B loci, the most striking difference is greater representation of the API and AFA populations by the Vendor 1 standard panel by 9.1% and 6.2%, respectively. However, Vendor 2 better represents the HLA-C alleles of all ethnic populations, with 14.0% increased coverage for the AFA population compared to Vendor 1. Finally, the greatest benefit in HLA-DRB1 coverage was seen in the API and HIS populations with a respectively increased coverage of 6.5% and 5.1% when the Vendor 2 panel was used. High resolution typing of 60 deceased donors showed that 28.3% of donors had at least one HLA allele that was not represented in either vendor’s reagents. Molecular modeling showed that many of these HLAs had potential epitopes that were not represented in other HLAs in the reagents.
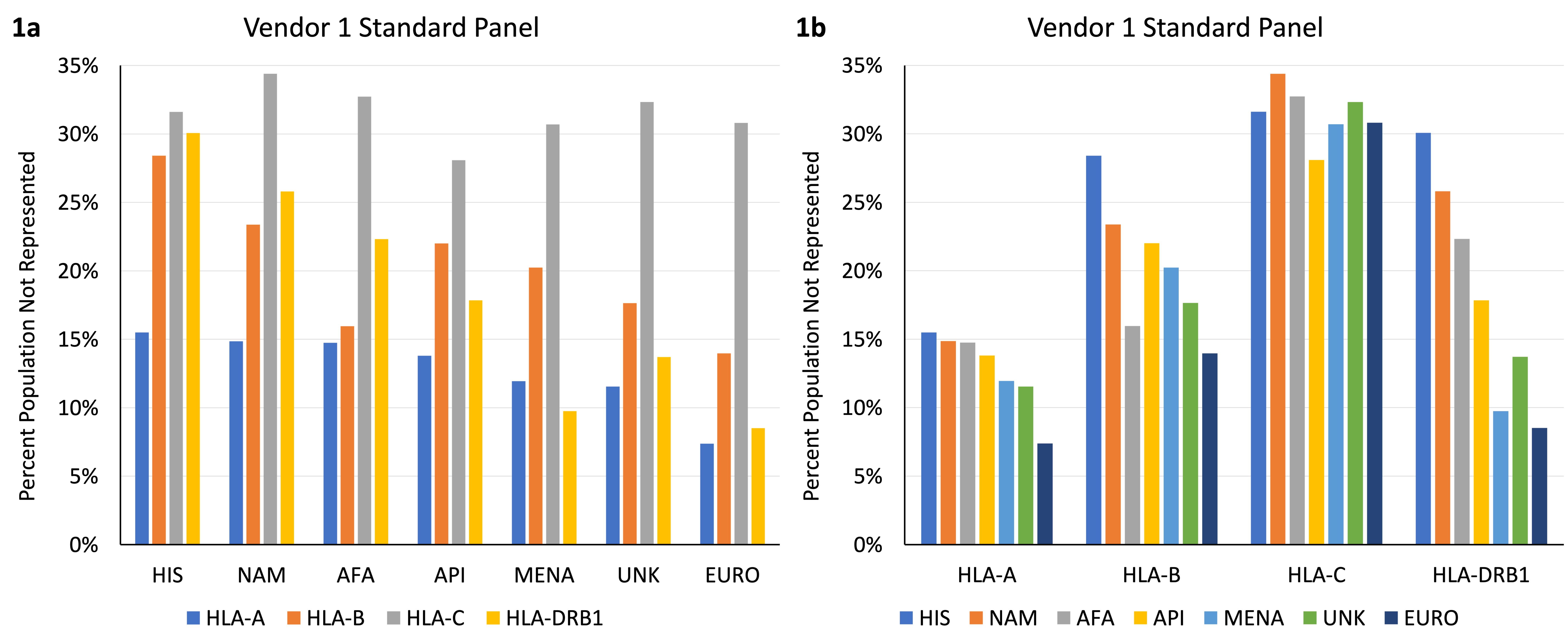
Conclusion: Antibody reagents do not cover all HLA alleles and may not be sufficient in ruling out the presence of HLA antibodies, since every ethnic population has HLA antigens that are not represented in single antigen reagents. This risk is increased in non-European populations. Different vendors choose different antigens to cover, and thus have different strengths with different ethnic populations.

right-click to download