
Lucino Bahena Carrera, Mexico has been granted the Emerging Economy Congress Scientific Award

High intrapatient variability tacrolimus's levels is associated with post-transplant diabetes mellitus in kidney transplant, a mexican cohort
Lucino Bahena Carrera1, Héctor Faustino Noyola Villalobos1, Ricardo Mendiola Fernández1, Miguel Eduardo López Chico1, Alexis Aguilar Marcial1.
1Nephrology and Trasplant, Central Military Hospital, Mexico city, , Mexico
Introduction: Porrini E showed that tacrolimus represents a risk factor for post-transplant Diabetes Mellitus (PTDM) development, increasing prediabetes incidence by 33% 1 year post-transplantation. Several mechanisms have been implicated in the association of calcineurin inhibitor and PTDM: decreased insulin secretion, glucose intolerance, reduced pancreatic beta cell mass and decreased insulin gene expression. DIRECT study (Diabetes Incidence after Renal Transplantation) showed the incidence in 73 CsA patients (26%) and 96 Tac patients (33.6%, p = 0.046). By the other side, Malik RF et al mention that FK levels isn´t a risk factor for the development of PTDM.
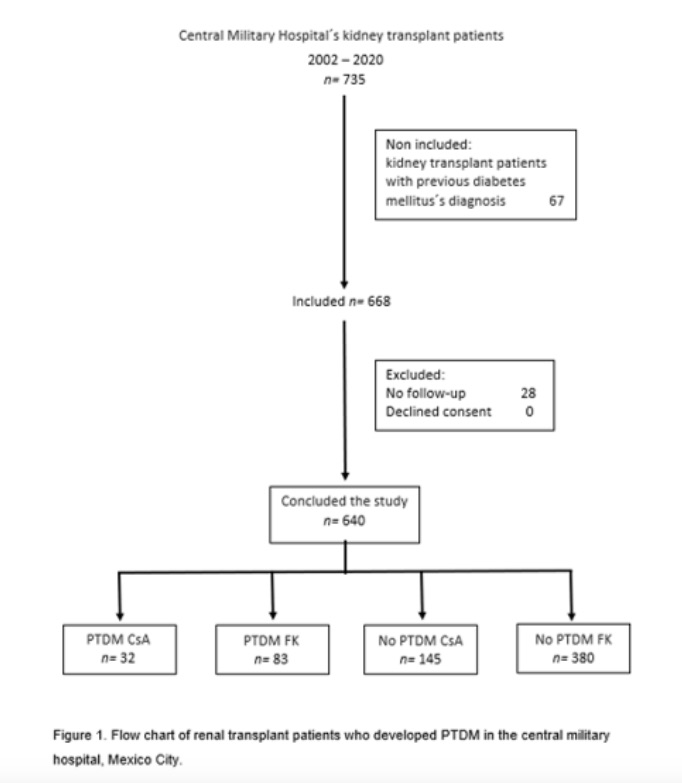
Method: A retrospective study was performed. All patients who received living or deceased-donor kidney transplant in the study period 2002 to 2020 was included and measured Tac/CsA and glucose level at months 0,3,6,9, and 12. Hb1Ac was also determined at 6 and 12 months. Patients who did not have at least 12 months post-transplant follow-up were excluded. PTDM diagnosis was made according the American Diabetes Association (ADA). Intrapatient Variability (IPV) coeficient was estimated by calculating the CV according to the following equation: CV (%) = (SD/mean Tac trough concentration) ×100. Mean concentrations were calculated using all outpatient Tac concentrations between 1 and 12 months. Recipients were separated into 2 groups, low IPV and high IPV, according to the CV cutoff= 37.31% (which is CV median value in the whole cohort).
Results: 640 patients were included; 69.4% were transplanted from living related donors; most frequent CKD etiologies were ND and CNG with 33.3%, 30.3% respectively. 64.4% of the transplant recipients were induced with Basiliximab and 1-year postransplant time, 463 patients (72.3%) were on tacrolimus as maintenance immunosuppression and 27.7% on CsA. The mean age recipients was 38.32 (±13.66) years old. Cr mean 1-year postransplant time was 1.39 (±1.19) mg/dL. There were no statistical differences in mean oral steroid dose between groups. Mean levels FK and CsA were 12.41 (±5.31) and 234.34 (±87.80) ng/mL and 9.13 (±5.3) and 194.38 (±92.44) ng/mL in the PTDM and whitout PTDM groups, respectively (p >0.05). 116 patients did met PTDM criteria (18.1%) within first year after transplantation; 55.1% patients were treated with metformin and 33.6% patient with basal insulin. Patients who had tacrolimus high IPV coefficient developed higher PTDM than those with low variability with statistically significant difference (43.22% vs 29.99%, p<0.05). The student's t test value to compare the IPV was 0.03; ANOVA p= 0.00. Our PTDM incidence was lower than other hispanic multicenter cohort.
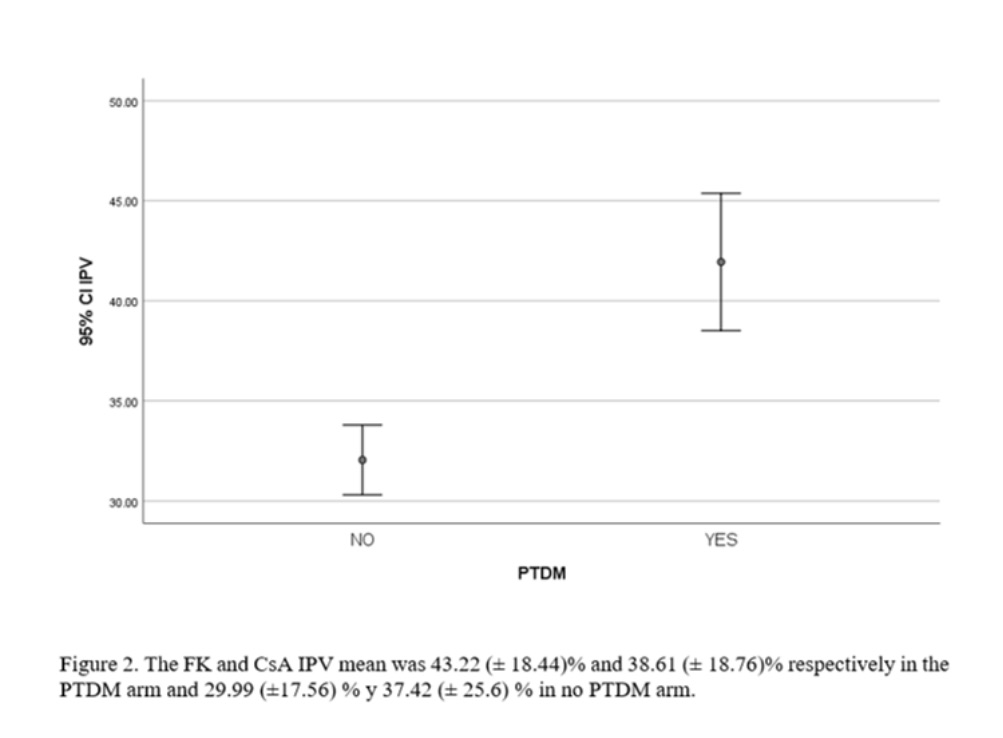
Conclusion: High IPV tacrolimus´s levels proved to be another risk factor for the development of PTDM. The use of prolonged-release medications can be a measures to maintain stable serum values and reduces this complication. Other prospective studies should be carried out to verify the results found.

right-click to download