
Learning from the learning curve: the personal database of an entry-level transplant surgeon as a tool to improve outcomes
Alex Zendel1, Megan Lombardi1, Betelhme Gebre1, Alexander Toledo1, David A Gerber1.
1Division of Abdominal Transplantation, University of North Carolina at Chapel Hill School of Medicine, Chapel Hill, NC, United States
Background: The transition from a trainee to an independent surgeon is a long and gradual process. We present an example of using of personal cases database as a self-learning, practical tool for a beginning transplant surgeon for improving outcomes.
Methods: Data from a single surgeon post-fellowship initial experience in deceased donor kidney transplants, including donors, recovery and preservation features, recipient demographics and pre-operative characteristics, peri-operative surgical data, and short-term outcomes, has been systematically collected. After the completion of the first 20 cases (Group 1), the data analysis was performed, resulting in subsequent modification of surgical planning and technique. The data from the following 20 cases (Group 2) was analyzed and compared to assess the effect of changes made.
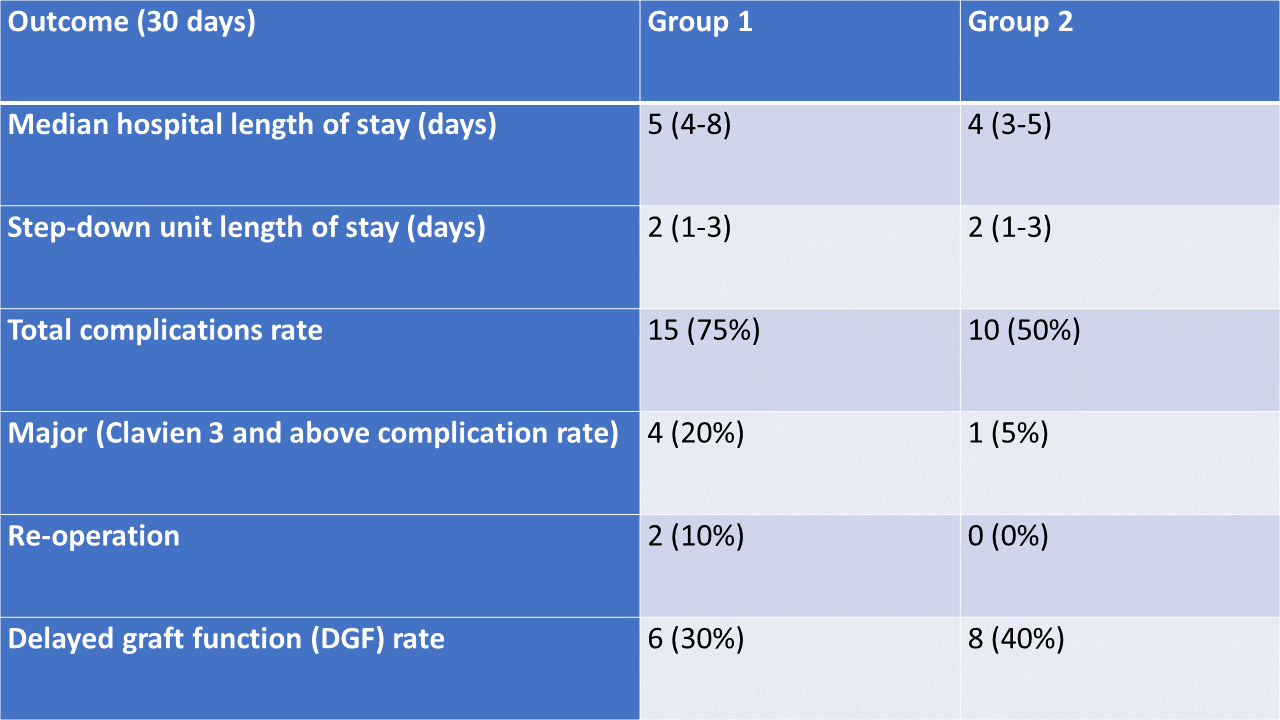
Results: No difference was observed in recipient age, sex, body mass index BMI and calculated peri-operative risk. Kidney donor profile index (KDPI) and cold ischemia time (CIT) were higher in group 2 (37% vs 44% and 15 vs 17 hours, group 1 and 2, respectively). Operative time and warm ischemia time (WIT) improved in group 2 (4 vs 3.3 hours and 39 vs 35 minutes, group 1 and 2, respectively). Blood loss was not different between the groups (100 ml). Group 2 had improved hospital length of stay, total and major complication rates, and re-operation rate (Table). The delayed graft function (DGF) rate was higher in group 2. All patients with DGF had a recovery of graft function and all 40 patients maintained preserved graft function during the median follow-up of 6 months.
Discussion: Based on data analysis from the first 20 transplant cases, modifications were made to the surgical technique, such as exposure improvement, prompt placement of anastomotic sutures to reduce the WIT, use of topical cooling, and optimization of vascular clamps. That led to an observed improvement in perioperative and short-term outcomes in the next 20 cases. The higher rate of DGF can be explained by longer CIT in Group 2. We suggest an entry-level transplant surgeon choose a structural approach, including formulating his own standard surgical plan, personalizing the surgical instruments kit, improving the teamwork by instructing the surgical team pre-operatively, and debriefing at the end. In our opinion, one of the most important tools for improving personal experience and outcomes would be the use of personal cases database, analyzing the results of a certain number of cases, and modifying and improving surgical planning and technique.

right-click to download